Thermosemiotics of chronic tonsillitis
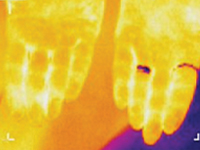
Research Objective – to develop thermosemiotics of chronic tonsillitis by determining specifics of infrared waves in the submandibular region and on the palms, knees and in the center of foot vault in healthy people and comparison of the obtained results with the corresponding indices of patients with chronic tonsillitis. Most common pathogens in infectious tonsillitis are Streptococcus spp. Tonsillitis infrequently develops on the background of acute respiratory disease, but usually manifests itself as a separate disease. Suppression of local immune response on cold exposure, malnutrition, physical exhaustion, blockage of nasal pathways by adenoid tissue, chronic sinusitis, deviation of the nasal septum, chronic rhinitis are favorable set ssup for tonsillitis formation [1-3]. In clinical practice, it is often necessary to distinguish acute tonsillitis from chronic, because they are fundamentally different diseases. Recurrent acute tonsillitis that is frequently undertreated is commonly seen as preceding factor in development of chronic tonsillitis. Follicular form of tonsillitis is considered most unfavorable as it leads to scar formation in lymphoid tissue therefore diminishing its protective properties. Tonsillolith are formed consisting of desquamated epithelium, microbes, inflammatory exudate. They are difficult to evacuate and causing lacunar expansion, formation of retention cysts [4, 5]. Tonsilitis is notorious for its complications, such as myocarditis, rheumatic diseases, nephritis. Exacerbation may occur on the background of chronic inflammatory process. Therefore, special attention needs to be directed to patient reported history, particularly frequency and duration of exacerbations. Exacerbation of chronic tonsillitis is accompanied by symptoms of general intoxication – subfebrile temperature, pain in joints, decreased tolerance to physical exertion, fatigue. The tonsils, as a rule, are enlarged, have submucosal purulent follicles (however, in the absence of signs of acute tonsillitis, hyperemia and inflammatory infiltration may be present), caseosus-purulent masses in cicatricial lacunae. Regional lymph nodes are enlarged, dense, sometimes painful. Tonsil-cardial syndrome is often observed with subjective sensations of pain in the region of the heart, heart intermission, palpitation. There may be vasomotor symptoms – pallor or hyperemia of the skin, xerodermia or increase perspiration functional heart murmurs, myocarditis [4].Research Objective – to develop thermosemiotics of chronic tonsillitis by determining specifics of infrared waves in the submandibular region, on the palms, in the projection of kneecaps, and in the center of foot vault both in patients with chronic tonsillitis and healthy persons.