Publications
Peer-reviewed clinical case reports

Postępowanie w dystocji barkowej u pacjentki rodzącej do wody - studium przypadku
The management in shoulder dystocia during water birth- case study.
GynecologyThis study describes a management of shoulder dystocia during water birth. It contains a guideline for the management of shoulder dystocia developed by the Obstetrics and Gynecology Ward and Chair in Tychy.

Izolowany nerwiakowłókniak splotowy ręki: opis dwóch przypadków. Propozycje diagnostyki i leczenia.
Isolated hand plexus neurofibroma: two case reports. Diagnostics and treatment proposals.
GynecologyNeurofibromas Plexiform neurofibromas are benign tumors of the peripheral nerve sheath. They can be found as single or multiple nodules, which are part of the of the clinical picture in any type of neurofibromatosis, and can become malignant. Neurofibromas arise from Schwann cells which are part of the nerves of the skin throughout the body, nerves innervating internal organs and cranial nerves. The most characteristic symptoms include the presence of scattered, elongated, resilient subcutaneous nodules. These are fibromas, histologically resembling individual neurofibromas, appearing along the the course of peripheral nerves or cranial nerves. They most often occur on the face and neck. Sometimes they lead to massive enlargement of a limb or other part of the body (neurofibromatous elephantiasis) [1,2]. Another equally common common symptom is skin discoloration, looking resembling coffee spots ("giant café-au-lait spot"), as well as freckle-like lesions localized around the axillae and axillary pits [3]. Neurological symptoms are associated with the compression of neurofibromas on adjacent structures. The patient then complains of neuralgia of the peripheral nerves. In the literature we can find isolated cases of neurofibroma plexiformis without any association with neurofibromatosis type 1 [4-6]. Treatment of patients with plexiform neurofibromas is not well defined defined and is mainly aimed at controlling symptoms. Surgical excision is the only available therapy, as there there are no drugs that can prevent their formation or treat them conservatively conservatively. At present, the results of surgical excision are not fully satisfactory, and these procedures can be complicated due to the size, location, condition of the vessels, involvement of the neural involvement, microscopic staging and high rates of tumor re-growth [7]. It should also take into account the fact that there are known there are many causes causing tumor-like lesions to neurofibromas . These include traumatic soft tissue injuries, arthritis, tendon diseases (e.g. tendinosis, tendon sheath inflammation, tendon rupture), non-neoplastic soft tissue lesions (e.g. ganglion, bursitis, granuloma) , and, less commonly, tumors and their metastases to soft tissues [8]. Focal lesions of soft tissues soft tissues are often the cause of pain and palpable tumor mass [9]. W these cases, especially in the early stages, accurate diagnosis is crucial, to establish a diagnosis and treatment strategy. Therefore, w when confronted with a focal tumor lesion the logical seems is to follow established algorithm of procedure. First, it should provide an accurate description of the lesion in correlation with the patient's age, location, type of involved tissue, the condition of the adjacent environment. For this purpose, in addition to detailed clinical examination, ultrasound should be performed of the occupied area, and if a bony lesion is suspected then an x-ray examination in two projections with adjacent joints. The advancement of bone lesions, it is necessary to deepening diagnosis through CT examination. However, lesion limited only to soft tissues on ultrasound will require MRI diagnosis, which will more accurately visualize the infiltration by its neighborhood. If imaging studies show a high probability of proliferative disease, an important diagnostic element is to obtain material for pathomorphologic examination, taken during open biopsy or oligobiopsy and establish the histological diagnosis [10]. If the neoplastic process is confirmed, it is always necessary to X-ray/CT scan of the chest, ultrasound/CT scan of the abdomen and even even PET to exclude metastases [11]. The second stage of the implemented algorithm dictates that treatment should be planned based on the answers to the following questions: - Is the lesion likely to be a normal variant, i.e., "leave me alone, don't touch me." lesion of a benign type, requiring no further imaging or supplies, but only observation? [12] - Does the lesion have features suggestive of an aggressive nature, and then how far advanced should be treatment? [13]. The heterogeneity of the clinical picture of unidentified focal nodular lesions in the metacarpal region, the variety of available methods of diagnosis do not make the task any easier the task, both at the stage of making the initial diagnosis and during communication between members of the interdisciplinary team, who, on more than one occasion, should handle the treatment. Therefore, it seems important to cooperate on the line of orthopedist-oncologist-pathomorphologist. Two cases of isolated neurofibromatosis of the palm of the hand are described below because of their uniqueness. The second of the described cases indicated an additional possibility of postoperative treatment of the patient in the form of prolotherapy injections to improve the function of the treated limb.
Mastektomia i jednoczasowa rekonstrukcja piersi u chorej na mięsaka gruczołu po przebytym skojarzonym leczeniu oszczędzającym z powodu raka
Mastectomy and immediate reconstruction at woman with breast sarcoma following breast connserving treatment due to cancer
GynecologyBreast sarcomas are rare, accounting for 1% of malignant gland tumors and less than 5% of all tumors mesenchymal neoplasms.1 The low incidence makes it difficult to conduct trials randomized clinical trials, and available data include descriptions of retrospective series and single cases. The number of known factors that increase risk of developing the disease is small. A genetic predisposition in the form of syndrome Li-Fraumeni (TP53 gene mutation) increases the risk of primary sarcomas also in the thoracic location.2 Chronic lymphedema occurring in some patients after axillary lymphadenectomy and axillary irradiation predisposes to lymphangiosarcoma in the affected arm (Stewart syndrome and Treves syndrome).3 Secondary sarcomas occasionally occur in breasts previously irradiated after breast conserving treatment (BCT), performed for breast cancer, the most common malignancy in women, and after radiation therapy administered for malignant granuloma.4 The cumulative risk of of radiotherapy-induced sarcoma (RIS) is 3.2 per 1,000 over 15 years vs. compared to 2.3 per 1,000 for primary sarcoma in a population without radiation therapy.5 Compared to women who were not irradiated, patients treated with radiation therapy for breast cancer, the risk of developing radiotherapy-induced hemangiosarcoma (radiotherapy-induced angiosarcoma, RIA) is five times higher 6 , in general, however, the possibility of of developing angiosarcoma after radiation therapy is low and, according to the literature literature, it is 0.03 - 0.2% in more than 10 years of follow-up.7,8 It should be clearly emphasized the benefits enjoyed by women with breast cancer due to radiation, an obligatory part of breast-saving treatment.9 There has been no correlation of the incidence of RIS with the use of chemotherapy.10 For the The diagnosis of radiotherapy-induced sarcoma can be made using criteria proposed by Cahan in 1948,11 as interpreted by Kirova15 (At that time, Cahan described more than a dozen cases of bone sarcomas in patients irradiated according to the treatment standards of the time for benign lesions and bone tuberculosis, the first point in the original description was the non-neoplastic nature of the lesion treated with radiation therapy)11: 1. History of treatment with irradiation 2. asymptomatic latency period between two cancers lasting several years 3. occurrence of sarcoma in a previously irradiated area, 4. Histopathologic confirmation of sarcoma as a second neoplasm.10,11,15 However Cahan described the latency period as "relatively long," amounting to more than 5 years in his paper, the literature a case has been described that appeared before a year, also described as a RIS (RIA).12 Among the histopathological types diagnosed among secondary sarcomas include angiosarcoma, hemangiosarcoma, leiomyosarcoma, malignant fibrous histiocytoma, liposarcoma, and fibrosarcoma. Also described were chondrosarcoma and osteosarcoma. RIS develop most often in the chest wall, less often in the parenchyma of the of the irradiated breast.10 The method of choice for patients with for breast sarcomas is excision of the tumor with a margin of healthy tissue. While in the case of primary sarcomas, follow-up treatment after sparing surgery often consists of irradiation of the operated area, when treating patients with for sarcoma occurring in a previously irradiated area, repeat radiotherapy of the of the same area is not recommended. The optimal type of treatment in such a case is mastectomy in this case.

Przykład postępowania w przypadku guza II kości śródstopia pierwotnie podejrzewanego jako przerzut raka pęcherzykowatego tarczycy 40 i 20 lat po całkowitej tyroidektomii
Example of management of metatarsal bone II tumor originally suspected of having metastatic thyroid follicular cancer 40 and 20 years after total thyroidectomy
GynecologyKnown There are many causes causing discomfort and nodular lesions in the metatarsal area and forefoot. They include These include traumatic soft tissue injuries i bones (e.g., sole plate tears, toe arthritis, arthritis, fractures fatigue, Freiberg fracture), tendon diseases (e.g. tendinosis, tendon sheath inflammation, tendon rupture), non-cancerous soft tissue lesions (e.g., ganglion, bursitis bursitis, granuloma, Morton's neuroma), and, less commonly, tumors and their metastases to soft tissues and bone [1]. Focal bone lesions are often an incidental result of imaging. Alternatively, they may be the cause of pain, a palpable mass or a fracture pathological [2].Most often patients associate these symptoms with trauma. In fact, trauma only draws attention to the the affected area, but does not cause the formation of a tumor. [5] In all these cases, especially in the early stages, accurate diagnosis is crucial, to establish further differential diagnosis and treatment strategy, so when confronted with a focal bone lesion, it is necessary to follow a logical management algorithm. First, it should provide description of the lesion in correlation with the patient's age, location, type of bone, cortical involvement, periosteal reactions, the condition of the adjacent soft tissue. W this for this purpose, it is necessary to x-ray of the involved area in two projections with adjacent joints. A deeper diagnosis is achieved by CT examination, assessing the advancement of the bone lesions and MRI, infiltrating adjacent soft tissues . If imaging studies show more advanced disease, an important diagnostic element is to obtain material for pathomorphology, taken during open biopsy or oligobiopsy, and establish the histological diagnosis [11]. W case of confirmation of a neoplastic process, it is always necessary to perform a examination X-RAY/CT chest, ultrasound/ CT of the abdomen, or even PET to exclude metastases [5]. The second step of the implemented algorithm dictates that treatment should be planned based on the answers to the following questions: - Is the lesion likely to be a normal variant, That is, "leave me alone, don't touch me," a lesion of a benign type, requiring no further imaging or supplies, but only observation? [3] - Does the lesion have features suggestive of an aggressive nature, and then whether further imaging is necessary, which technique best to use, whether a biopsy of the lesion is required and advanced treatment? [4]. Heterogeneity clinical picture of unidentified focal nodular lesions w metatarsal and forefoot, the variety of available methods of diagnosis do not make the task any easier, both at the stage of making the initial diagnosis, as well as during communication between members of the interdisciplinary team, which many times should deal with address treatment. The purpose of of this article is to present a similar situation using the case of a tumor of the distal epiphysis of the second metatarsal bone as an example, suspected of late, distant metastasis of thyroid cancer, never not confirmed in further studies, and suggestions for management diagnostic and therapeutic management. Cancer Follicular The thyroid gland (FTC - Follicular Thyroid Carcinoma) accounts for 10-20% of of all cancers of the thyroid gland. It is the second most common encountered thyroid cancer [6], and metastasis to the metatarsal bones and fingers are extremely rare.

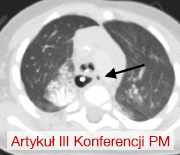
Nawracająca odma opłucnowa w przebiegu mukowiscydozy – trudności terapeutyczne. Opis przypadku.
Recurrent pneumothorax in course of cystic fibrosis – treatment challanges. Case report.
GynecologyCystic fibrosis (cystic fibrosis) is the most common genetic disease with autosomal recessive inheritance among the Caucasian population. The incidence varies from country to country. In Poland, it is about 1/2300 of live births. In its course, as a result of mutations on both copies of the CFTR (cystic fibrosis transmembrane conductance regulator) gene, which encodes a chloride channel, ion transport in all exocrine glands is disrupted, leading to dysfunction of key organs for survival, such as the pancreas, liver, lungs and intestines [1].Respiratory complications are the first cause of premature death in CF patients. Pulmonary manifestations of CF include hemoptysis, pneumothorax, chronic sinusitis and airway inflammation, bronchial dilatation, and respiratory failure, among others. Pneumothorax is the presence of air in the pleural cavity. Risk factors are associated with chronic infection with Burkholderia cepacia and Pseudomonas aeruginosa and the coexistence of other complications such as hemoptysis and pancreatic insufficiency [4]. Significant disease progression (FEV1 30%) [2] also favors the occurrence of this complication. Taking into account the criterion of time, we can distinguish the first case of emphysema, or recurrent emphysema, when the air leak reappears within 7 or more days after the previous episode. If the air leak persists for 5 or more days, we can recognize persistent emphysema (Shidlow 1993). Therapy can be divided into medical (oxygen therapy and observation) or surgical interventions. The latter group, which includes drainage, pleurodesis and pleurectomy depending on the course of treatment, is considered a more effective therapeutic option for patients with emphysema without significant concomitant lung disease. However, in CF-affected patients, it may complicate the lung transplant procedure in the future. There are no clinical trials available that reliably compare the efficacy and risk of complications of both types of interventions in CF patients [3-4]. An additional complication is that emphysema recurs in 50-90% of these patients, and in almost half of them it also occurs on the opposite side of the chest. Emphysema significantly worsens lung function, and the patient experiences shortness of breath and significant pain. If refractory to treatment, it is an independent indication for lung transplantation.[5]Here we present the case of a 16-year-old female patient with recurrent unilateral pneumothorax, in which, due to the severity of the disease, the diagnosis and therapeutic measures taken were fraught with numerous problems.

Skręt esicy u nastoletniego pacjenta
Sigmoid volvulus in an adolescent male patient
GynecologySigmoid volvulus (SV) is a condition where sigmoid colon twists or torsions about its mesentery. This disorder is rare in infants and children[1]. It usually occurs in adults, after the age of 40, more commonly in males[2]. SV leads to intestinal obstruction, which is often acute in children, whereas in adults it may be subacute or progressive. As a result of intestinal obstruction, the most common symptoms include abdominal pain, distention, vomiting and, in chronic cases, constipation. In Europe, Australia and the United States, the incidence of SV is very low. Nevertheless, SV remains the leading cause of acute colon obstruction in developing countries[3]. The diagnosis is based on clinical and radiological findings and is more difficult to establish in children compared to adults[4], and a correct diagnosis can be easily missed or delayed[4]. We present a case report with exceptional quality CT images and 3D reconstructions.

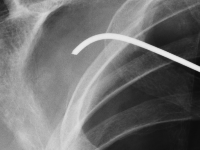
Migracja złamanego drutu Kirchnera po zespoleniu zwichniętego stawu barkowo-obojczykowego – opis przypadku.
Migration of a Kirschner wire used in fixation of acromioclavicular joint dislocation – case report.
GynecologyDislocation of the acromioclavicular joint refers to complete or partial misalignment of the articular surfaces of the neighbouring scapula and clavicle [1]. It is an injury which often occurs in contact sports, such as football, judo, rugby and many more. It is also a relatively common injury in daily activities, as a result of falling during a walk or falling off a chair with impact on the shoulder girdle [2], [3].<br />Depending on the grade of the injury, recommended approaches vary from conservative treatment (grade I and II) to surgical treatment (above grade III).<br />Conservative treatment recommendations are: cooling, painkillers and limb elevation. Surgical treatment consists of surgical stabilisation of the dislocation. There are many techniques and methods to fixate the injury, including: Kirschner wires, using TightRope, double Endobutton, MINAR, Copeland and Kessel, Waver and Dunn or dedicated plates [3], [4].<br />

Staw rzekomy w wyniku złamania trzonów kości podudzia u dziecka – opis przypadku
Pseudoarthrosis after tibia and fibula shaft fracture in a child – case report
GynecologyJest to rzadki przypadek, w którym pierwotnie zdiagnozowane przerzuty FTC do kości śródstopia nie zostały potwierdzone w dalszej diagnostyce. W związku z tym wykonano jedynie resekcję guza. Diagnostyka pooperacyjna opierała się na wielokrotnych, dokładnych badaniach histopatologicznych wycinków pobranych w trakcie operacji, co wykluczyło niekorzystne rozpoznanie. Dzięki temu uniknięto amputacji stopy.

Przyzwojak u 41-letniej kobiety - rzadki nowotwór przestrzeni zaotrzewnowej
Paraganglioma in a 41-years old woman: a rare neoplasm of the retroperitoneal space
Gynecology<p>Paraganglioma(Latin: paraganglioma) is a rare, mostly benign neuroendocrine tumor originating from the paraventricular bodies of the parasympathetic and sympathetic nervous systems. The 2013 National Cancer Registry did not find any data on the incidence of this tumor in Poland [1]. The histopathological structure and symptoms of the tumor often resemble pheochromocytoma. It can be said that pheochromocytoma is a special type of chaperone tumor. Chaperones originating from the parathyroid bodies of the parasympathetic nervous system are usually located near the large vessels of the head and neck (bifurcation of the common carotid artery-the most common location) [2], while chaperones from the sympathetic nervous system chaperones occur along the sympathetic trunk located adjacent to the vertebral column, abdominal aorta and inferior vena cava [even aortic glomerulus (Zuckerkandel's organ) lying on either side of the aorta, just above its bifurcation-the most common location].</p><p>Parenomas are neoplasms of old age, with peak incidence in the 5th and 6th decades of life. In about 10% of cases, they occur familially, being part of such genetically determined syndromes as [3]:</p><p>- von Hippel-Lindau syndrome</p><p>- multiple endocrine adenocarcinoma syndrome types 2A and 2B</p><p>- Carney syndrome</p><p>Diagnosis of chaperones is not straightforward, as these tumors are rare. In cases where the tumor is hormonally active, there are symptoms associated with high levels of catecholamines in the blood (accelerated heart rate, increased blood pressure, hot flashes, headaches). When a hormonally active tumor is absent, symptoms may result from tumor growth in a specific location (dull pain in the lumbar region). Most often, however, chaperones are diagnosed incidentally in a neck or abdominal and pelvic ultrasound performed for other reasons or as an annual prophylaxis (the tumor diagnosis is then confirmed on CT).</p><p>Tumor fine-needle biopsy is unlikely to be performed due to the rich vascularization of the tumor and the associated risk of bleeding.</p><p>Because of the rarity of chaperones, there are no established diagnostic and therapeutic algorithms.</p><p>Treatment consists of surgical removal of the tumor. In cases where the location of the tumor does not allow surgical removal, radiation therapy is applicable.</p><p></p><p>Rocalization is generally very good. If the tumor is completely removed, the cure is complete.</p>
Ciało obce w klatce piersiowej
A foreign body in the chest
GynecologyPatients with pneumothorax constitute a significant percentage of all hospitalizations in general surgery departments. Pneumothorax can be spontaneous, most often caused by pulmonary emphysema, or post-traumatic, primarily resulting from chest wall contusion. A specific type of pneumothorax is the iatrogenic variety, which can generally be classified as post-traumatic.

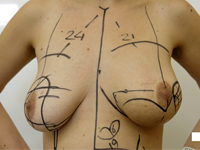
Rak piersi w ciąży – propozycja leczenia operacyjnego z jednoczasową rekonstrukcją gruczołu piersiowego
Breast cancer in pregnancy – a proposal of surgical treatment with immediate reconstruction of breast
GynecologyBreast cancer in pregnant women includes cases in which breast cancer develops during pregnancy or within 12 months of delivery and occurs in 1 to 3 in 10,000 pregnancies, representing 0.2–4% of all breast cancers [1]. Statistically, it most often occurs in women aged 50–69 years, while it is not common in women under 40 years of age. However, recent observations indicate an increase in the number of breast cancer cases diagnosed before menopause [2]. The trend in the incidence in premenopausal women (20–49 years of age) is upward, and over the last three decades, the incidence in this age group has almost doubled [3]. This indicates an increase in the number of cases due to the clearly visible tendency to become pregnant later in the reproductive years. The average age of breast cancer patients at the time of pregnancy is 33 years [4]. An increased risk of developing the disease also applies to women who carry constitutive mutations in the BRCA1 gene and those with a family history of breast cancer. Diagnosis and treatment of cancer patients during pregnancy are difficult due to nonspecific symptoms overlapping with pregnancy-related ailments and symptoms. Once a cancer diagnosis is confirmed, decisions regarding further treatment should be aimed at both optimal maternal treatment and maintaining normal fetal development [5].
Lewostronna torakoskopia celem usunięcia uchyłka tchawicy i nawrotowej przetoki tchawiczo-przełykowej
Left thoracoscopic approach to remove tracheal diverticulum and recurrent tracheo-esophageal fistula
GynecologyEsophageal overgrowth is a rare congenital defect that still poses a challenge to the surgeon. Among the types of overgrowth, the most common is type III, characterized by the presence of an esophageal-tracheal fistula from the lower segment. The procedure involves closing the fistula and then anastomosing the two overgrown sections. In some cases, complications develop, among which the most common are esophageal stricture at the anastomosis site, leakage at the anastomosis site, and recurrence of esophageal-tracheal fistula. Case report: The authors present a description of the diagnosis and treatment of a girl operated on for esophageal overgrowth t. III, who developed a large tracheal diverticulum and recurrence of esophagotracheal fistula. The choice was unusual surgical access through the left pleural cavity using a thoracoscopic technique.