Publications
Peer-reviewed clinical case reports
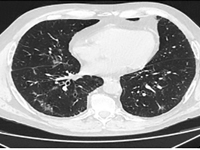
Infekcja SARS-CoV-2 u chorego na raka gruczołowego z mutacją w genie EGFR leczonego erlotynibem – opis przypadku
SARS-CoV-2 infection in a patient with adenocarcinoma with a mutation in the EGFR gene treated with erlotinib - a case report
Internal MedicineLung cancer accounts for the largest number of cancer deaths worldwide [1]. Despite advances in treatment, incidence and mortality rates continue to rise. A 2018 GLOBOCAN analysis reported 2.09 million new cases of lung cancer and 1.76 million deaths from lung cancer worldwide [2]. There are two main histological types: small cell lung cancer (DRP) and non-small cell lung cancer (NDRP). NDRP accounts for about 85% of all lung cancer cases. It includes various subtypes such as adenocarcinoma, squamous cell carcinoma and large cell carcinoma. The most common subtype is adenocarcinoma accounting for 45% of NDRP cases. The most important risk factor for developing lung cancer is smoking, especially among the male population. The use of filtered cigarettes, which reduce the amount of tar entering the lungs, correlates with an increase in the incidence of lung adenocarcinoma, which is associated with stronger inhalation of carcinogens into the fine airways. Other compounds that may have an effect on cancer development are asbestos, radon, nickel, cadmium, chromium, silica and arsenic. The development of molecular studies at the beginning of the 20th century made it possible to identify the genetic basis of the disease by demonstrating the presence of mutations or rearrangements of TP53, MYC, BCL2 genes in small cell carcinoma and EGFR, KRAS, MET, BRAF, NTRK, ROS1, ALK, RET, PIK3CA genes in non-small cell carcinoma [3]. The percentage of non-squamous NDRP patients with mutations in the gene for the epidermal growth factor receptor (EGFR) is 10-15 (in Caucasian patients) to more than 40% (in Asian patients) [4]. A deletion in exon 19 and a substitution at codon 858 (L858R) in exon 21 account for 80-90% of mutations within the tyrosine kinase coding domain of the EGFR gene [4]. Lung cancer manifests as cough, hemoptysis, chest pain, shortness of breath and/or hoarseness. In the case of adenocarcinoma, brain metastases manifesting as headache, vomiting, visual field disturbances, seizures or neurological deficits are common. After appropriate laboratory and imaging tests and histopathological evaluation, it is possible to assess the histological type and stage of the cancer. Depending on the patient's general condition, tumor stage and concomitant diseases, different treatment methods are used. For low-grade cancer (stages I, II and IIIA), surgery is used, often in combination with chemotherapy and radiation therapy. For stage IIIB patients, the therapy of choice is chemoradiotherapy, and if chemoradiotherapy is not available, the treatment is the same as for patients with generalized NDRP. Therapy for patients with distant metastases (stage IV) is aimed at reducing the discomfort and symptoms of progressive disease and prolonging life. For this purpose, chemotherapy, immunotherapy or molecularly targeted therapy are used [5]. Molecularly targeted therapy for lung cancer with EGFR gene mutations is made possible by the use of tyrosine kinase inhibitors (IKTs). IKTs inhibit intracellular phosphorylation of EGFR which leads to the arrest of cell differentiation, proliferation and angiogenesis. EGFR IKTs are divided into three generations. Erlotinib and gefitinib are the first-generation reversible IKTs. They are effective in the presence of the most common mutations in exon 19 and 21. Second-generation irreversible IKTs, which include afatinib and dacomitinib, show a broader spectrum of action. They block the transmission of signals formed by ErbB1 (EGFR), ErbB2 (HER2), ErbB3 and ErbB4 receptors, and can be effective in the presence of rare mutations in exons 18, 19, 20 and 21. It is possible to acquire resistance to first- and second-generation IKTs. Ozymertinib, an irreversible third-generation IKT, by acting on cells with the T790M mutation in exon 20 of the EGFR gene, overcomes resistance to treatment with older-generation EGFR IKTs, but can also be used in 1st-line treatment in NDRP patients regardless of the type of mutation in exons 18-21 of the EGFR gene [6]. The global COVID-19 pandemic poses a therapeutic challenge to healthcare, especially among oncology patients. A retrospective analysis from Wuhan showed that the risk of COVID-19 infection was 2.31 times higher among cancer patients than in healthy individuals. Smoking, age, male gender, cancer status, poor performance status (≥2 on the ECOG scale) and treatment with hydroxychloroquine with azithromycin were risk factors for increased 30-day mortality among COVID-19 patients [7]. Hospital visits during the pandemic and the use of immunosuppressive medications are major contributors to COVID-19 infection in lung cancer patients [8]. A study conducted in China, showed that NDRP patients over 60 years of age are particularly vulnerable to COVID-19 infection and a more severe course of the disease. Many respiratory symptoms in COVID-19 i.e. shortness of breath, cough, fever overlap with those of lung cancer. This creates a difficulty in differential diagnosis between the two disease entities. The diagnosis of COVID-19 is usually made on the basis of clinical history and PCR test and/or antigen test in a sample from nasopharyngeal secretions. Recognition of typical lesions seen on chest CT scan is also helpful. Multifocal opacities of the frosted-glass type with predilection for the lower lobes are present in 75% of patients [9]. A study conducted in New York among lung cancer patients with concurrent SARS-CoV2 infection showed the need for hospitalization in 62% of patients, 21% of whom required ICU hospitalization. Of the 102 patients participating in the study, 25% died. Survival was more dependent on the comorbidity of COPD (chronic obstructive pulmonary disease) and smoking than on tumor histology or PD-L1 (programmed death ligand 1) expression on tumor cells [10].

Radykalna radioterapia konformalna w leczeniu nawracającej, pozasutkowej postaci choroby Pageta - opis przypadku.
Radical conformal radiotherapy in treatment of recurrent, extramammary Paget disease - case report.
Internal MedicineDisease Paget's disease is a rare neoplastic process originating in the glands of the apocrine and eccrine glands of the skin [1]. A distinction is made between the mammary Paget disease (MPD) form and the extramammary Paget disease (EMPD), accounting for 90% and 10% of all cases, respectively Paget disease [2]. The incidence of EMPD in the European population is estimated to be is estimated at 0.7 per 100,000 people/year [3]. EMPD is more often diagnosed in women, particularly Caucasian, between the ages of 50 and 80. [4], in whom it mostly localizes on the vulva and perineum and in the perianal area, while in men on the penis and scrotal sac [5,6]. The symptoms of the disease are uncharacteristic, which in most cases makes it difficult to make a correct diagnosis and thus prolongs the time to start treatment. Only histopathologic examination of the excised lesion allows a correct diagnosis and an assessment of the degree of invasiveness of the process [6]. The primary method of treatment remains radical surgery [7]. Due to the high recurrence rate [4,8], some patients require follow-up treatment [6]. In cases ineligible for surgery, local or systemic chemotherapy or radiation therapy is used [9,10].Given the very rare occurrence of the disease, the lack of established treatment regimens, observed failures and subsequent attempts at surgical intervention, the case presented here is an example of the possibility of treating EMPD with ionizing radiation.
Gdy Twój pacjent śpi za dużo, czyli zaburzenia świadomości u pacjenta geriatrycznego – opis przypadku
When your patient sleeps too much, disturbance of consciousness in the case of a geriatric patient – case report
Internal MedicineIn The world, including Poland, has seen a systematic increase in the share of the general population of elderly people. The aging of the population and the associated increase in the number of geriatric patients now represents another of the challenges to be met by 21st century medicine. Patient A geriatric patient, as defined by the WHO (World Health Organization Organization), is a patient who has reached at least 60 years of age. The person under study is usually accompanied by a significant amount of illness, which is typical of old age and coexists with the risk of sudden deterioration of health or death [1]. In line with the need, a number of solutions are being implemented around the world, leading to the to improve the branch of medicine that is geriatrics. Comprehensive assessment geriatric assessment (Comprehensive geriatrc assessment, CGA) is a tool that consists of a set of scales and tests that allow a holistic assessment of patients facilitating the detection of the cause of deterioration and the selection of optimal therapy. A complete patient assessment, depending on the patient's clinical condition, takes between 30 to 60 minutes [2]. Comorbidities and medications taken by geriatric patients geriatric patients often require significant modification of generally accepted standards of treatment. A large number of emergencies in elderly patients proceed with disturbances of consciousness. Difficulties in correctly perceiving the of the surrounding world that patients encounter greatly complicate the the ability to accurately take a medical history, as well as conduct a physical examination and implement appropriate diagnostic and therapeutic measures.
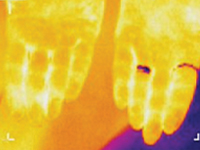
Termosemiotyka przewlekłego zapalenia migdałków
Thermosemiotics of chronic tonsillitis
Internal MedicineResearch Objective – to develop thermosemiotics of chronic tonsillitis by determining specifics of infrared waves in the submandibular region and on the palms, knees and in the center of foot vault in healthy people and comparison of the obtained results with the corresponding indices of patients with chronic tonsillitis. Most common pathogens in infectious tonsillitis are Streptococcus spp. Tonsillitis infrequently develops on the background of acute respiratory disease, but usually manifests itself as a separate disease. Suppression of local immune response on cold exposure, malnutrition, physical exhaustion, blockage of nasal pathways by adenoid tissue, chronic sinusitis, deviation of the nasal septum, chronic rhinitis are favorable set ssup for tonsillitis formation [1-3]. In clinical practice, it is often necessary to distinguish acute tonsillitis from chronic, because they are fundamentally different diseases. Recurrent acute tonsillitis that is frequently undertreated is commonly seen as preceding factor in development of chronic tonsillitis. Follicular form of tonsillitis is considered most unfavorable as it leads to scar formation in lymphoid tissue therefore diminishing its protective properties. Tonsillolith are formed consisting of desquamated epithelium, microbes, inflammatory exudate. They are difficult to evacuate and causing lacunar expansion, formation of retention cysts [4, 5]. Tonsilitis is notorious for its complications, such as myocarditis, rheumatic diseases, nephritis. Exacerbation may occur on the background of chronic inflammatory process. Therefore, special attention needs to be directed to patient reported history, particularly frequency and duration of exacerbations. Exacerbation of chronic tonsillitis is accompanied by symptoms of general intoxication – subfebrile temperature, pain in joints, decreased tolerance to physical exertion, fatigue. The tonsils, as a rule, are enlarged, have submucosal purulent follicles (however, in the absence of signs of acute tonsillitis, hyperemia and inflammatory infiltration may be present), caseosus-purulent masses in cicatricial lacunae. Regional lymph nodes are enlarged, dense, sometimes painful. Tonsil-cardial syndrome is often observed with subjective sensations of pain in the region of the heart, heart intermission, palpitation. There may be vasomotor symptoms – pallor or hyperemia of the skin, xerodermia or increase perspiration functional heart murmurs, myocarditis [4].Research Objective – to develop thermosemiotics of chronic tonsillitis by determining specifics of infrared waves in the submandibular region, on the palms, in the projection of kneecaps, and in the center of foot vault both in patients with chronic tonsillitis and healthy persons.

Wpływ diety wegetariańskiej na INR u pacjentki leczonej antykoagulantami
Effect of vegetarian diet on INR in patient treated with anticoagulants
Internal Medicine<p>Warfarin sodium (Latin: Warfarinum natricum), found under the trade name Warfin, is an effective anticoagulant used in the prevention and treatment of thrombosis. It is widely used after cardiac surgery, especially after implantation of an artificial heart valve prosthesis. Warfin's role is to prevent blood from clotting in the prosthesis and valve components and to help dissolve any clots that form.</p><p>Patients must continue anticoagulant treatment for the rest of their lives. They also remain under the constant medical care of the cardiology clinic. In general, they should monitor the prothrombin time (PT), or the time of blood clot formation, every 4-6 weeks to see how the clotting factors that go into the so-called prothrombin syndrome are working. The result is presented under the name International Normalized Ratio (INR) (<i>Enternational</i><i>Normalized Ratio)</i> [1]. In order to maintain stable blood density values, patients should adhere to a well-balanced diet, thus ensuring that the body receives the recommended daily dose of vitamin K contained in foods. Too high a dose of vitamin K in relation to the body's needs can significantly affect the INR value in the blood tested and create difficulties in selecting the antivitamin K dose [2].</p><p></p><p>There are three classified forms of vitamin K: K1 and K2 - derived from a natural source, and K3 which is a synthetic chemical compound. Vitamin K1 (phylloquinone) is synthesized exclusively in plants and taken with food, while K2 is a group of compounds known as menaquinones (MK-n) [3]. These compounds are synthesized by intestinal bacteria. They are mainly found in animal products, including those that are fermentable (Table 1).</p><p>Table 1.</p><p>Recommendations from the FAO (<i>Food and Agriculture Organization of the United Nations</i>) and WHO (<i>World Health Organization</i>). <i>World Health Organization), </i>for sufficient intake of AI (<i>Adequate</i><i>Intake</i>), expressed in μg of phylloquinone/os/d since 2008, have not changed and are 65 μg of phylloquinone/os/d for women ≥ 19 years of age while 55 μg of phylloquinone/os/d for men ≥ 19 years of age [5]. It is now accepted that the therapeutic INR for anticoagulant treatment in patients after artificial valve surgery should be in the range of 2.5 - 3.5 regardless of gender [6, 7]. The clinical efficacy of Warfin depends on the plasma vitamin K concentration, which is influenced by the amount of vitamin K ingested through food and from supplementation. The U.S. government agency FDA (<i>English </i><i>Food and Drug</i><i>Administration)</i> reports that a daily vitamin K intake of 400 μg or more can completely nullify the anticoagulant effects of Warfin taken by the patient [8, 9].</p><p>Selecting the right vitamin K-containing foods and distributing them in meals is a major challenge for the dietitian. Taking into account the patient's general condition and his or her age, gender, weight, comorbidities, other medications and supplements he or she is taking, as well as specific behavioral behaviors (diet, exercise), the dietitian can properly tailor an individual nutrition plan for a specific patient. The more information the nutritionist receives, the more accurate the result of his work will be. Green parts of vegetables and fruits are characterized by a high content of vitamin K1 (phylloquinone), so when establishing a diet plan for a patient, this factor should be taken into account first and foremost.</p><p></p><p>Vitamin K is also involved in bone metabolism. Long-term use of Warfin may disrupt the homeostasis of calcium metabolism in the patient's body, resulting in osteopenia and, consequently, osteoporosis. However, these are remote consequences. Additional factors such as age, gender, physical activity, genetic conditions may contribute to their occurrence [10].</p><p>An important element is the absorption of vitamin K in the body. The absorption of phylloquinone requires the cooperation of bile and pancreatic juice. It is a fat-soluble vitamin, so adding it to a meal results in higher absorption. Vitamin K is absorbed in the small intestine and is stored in the liver. There are differences between the absorption of vitamin K1 and K2. The former is absorbed only 10-15% of the total amount of this vitamin taken in with food, while K2 is absorbed almost completely and has a long biological half-life [10]. In the overall picture, vitamin K modifies coagulation stability, but it should not be excluded from the patient's diet because it is essential for the normal functioning of the human body. In addition to its involvement in the process of blood coagulation, it is involved in the maintenance of proper bone tissue homeostasis and in the proper functioning of the nervous system and brain function.</p><p></p><p>It can be assumed that a properly balanced dietary plan will contribute to the maintenance of normal concentrations of coagulation factors when confronted with anticoagulants and minimize fluctuations in the blood coagulation index.</p>

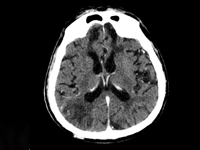
Problemy diagnostyczne oraz postępowanie terapeutyczne w przypadku neurokiły
Diagnostic problems and therapeutic procedures in the case of neurosyphilis
Internal MedicineCurrently, syphilis is a growing epidemiological problem, as evidenced by the growing number of new infections, also in Poland [1]. A negative phenomenon is the increasing incidence of late-stage Treponema pallidum infections, including syphilis of the central nervous system (CNS) [2]. In advanced stages of syphilis, and especially in neurosyphilis, the risk of permanent complications increases, including tenesmus dorsi, progressive paralysis, stroke, and others [3]. CNS syphilis poses a significant diagnostic challenge because the symptoms of infection can mimic other primary CNS diseases or systemic diseases with secondary CNS involvement. Therefore, it is often called "the great imitator" [4, 5, 6, 7].

Wewnątrzmaciczne zahamowanie wzrastania płodu w przebiegu Zespołu Silver-Russella - opis przypadku
Intrauterine growth restriction in the course of Silver-Russell syndrome - a case report
Internal Medicine<p>Intrauterine fetal growth restriction (IUGR) is one of the most serious complications of pregnancy. It affects an average of 8% of live-born newborns in developed countries, and up to 15-20% in developing countries[1, 2, 3].</p><p>It is associated with an increased rate of intrauterine deaths and pregnancy complications, including preterm deliveries and perinatal deaths. In children, abnormalities in psychophysical development and a higher incidence, including in adulthood, of conditions such as obesity, diabetes, and metabolic syndrome are observed[1, 2, 7, 8 , 9]. IUGR refers to the inability of the fetus to reach its full growth potential during intrauterine life [4, 5, 6]. Many times the term hypotrophy is used interchangeably. According to most authors, IUGR is diagnosed when two ultrasound measurements of the fetus show excessively slow growth rates and/or when birth weight/length is less than 2 SD ( standard deviations), or 10th percentile relative to gestational age. In severe forms, birth weight or AC ( abdominal circumference) correspond to values below the 3rd Centile. [6, 8]. The etiology of intrauterine growth retardation is multifactorial, and despite advances in medicine, it is often, even in 40%, impossible to identify . We distinguish maternal causes ( among others.: hypertension, kidney disease, cardiovascular disease, diabetes mellitus, thrombophilias, antiphospholipid syndrome, genetic factors, drugs), fetal(mainly genetic abnormalities, congenital malformations, intrauterine infections, metabolic blocks), placental (abnormalities in placental structure and capacity, pre-eclampsia), environmental (low socioeconomic status of the mother, stimulants, nutritional deficiencies) [1, 9, 10, 11, 12].</p><p>The management of suspected IUGR should include a thorough general medical and obstetric history, assessment of risk factors to identify pregnant women requiring enhanced surveillance, and detailed imaging and laboratory tests. Ultrasonography of the fetus (evaluation of anatomy, size , proportion, growth dynamics) is the primary diagnostic test. It is also necessary to monitor fetal well-being with cardiotocography (ktg), assessment of blood flow in selected vessels ( usg doppler), amniotic fluid volume and biophysical profile. Appropriate laboratory tests are performed to confirm or exclude maternal chronic diseases, intrauterine infections, pre-eclampsia, HELLP syndrome and other pregnancy pathologies that may affect growth disorders [12,13]. In the absence of a clear cause leading to IUGR, genetic testing is important. Maternal genes are believed to have a major impact on the baby's birth weight. However, also many chromosomal aberrations in the fetus are associated with intrauterine growth retardation [6, 12]. An example is Silver- Russell syndrome (SRS), which varies widely in the type of genetic alterations present and how they are inherited. Mutations affect chromosome 11, 7, among others, and are associated with characteristic phenotypic features, which include primarily bone lesions in the form of : scoliosis, limb length disproportion, toe fusion, elbow joint lesions. According to the literature, between 1:50,000 and 1:100,000 children are born with this syndrome [14, 15, 16].</p><p>The main goal of maternal and child care in pregnancy complicated by intrauterine fetal growth retardation is to ensure and strictly assess fetal well-being and to choose the optimal delivery date [6, 12].</p>.

Wykorzystanie Metod Radiologii Inwazyjnej w Leczeniu Pęknięcia Wątroby u Położnicy z Zespołem HELLP
Application of Methods of Invasive Radiology in Treatment of Liver Rupture in Woman after Delivery with HELLP Syndrome
Internal MedicineLiver diseases in pregnancy are rare. They are divided into pregnancy-related diseases, i.e., induced by pregnancy, and pregnancy-independent diseases, occurring as standalone conditions [2].<br />In addition to HELLP syndrome, pregnancy-related diseases include: hyperemesis gravidarum, intrahepatic cholestasis of pregnancy, preeclampsia and eclampsia, and acute fatty liver atrophy. These conditions affect and complicate approximately 5.5% to 13.5% of pregnancies. Preeclampsia, eclampsia, HELLP syndrome, and their complications, such as hepatic infarction and liver rupture/hematoma, are associated with hypertension in pregnancy. The most common conditions are preeclampsia and eclampsia, which affect 5-10% of pregnancies, and approximately 5% to 10% of these develop HELLP syndrome [3-5]. It is estimated to occur in approximately 6 pregnant women per 1000 pregnancies [2].<br />The concept and creation of the acronym HELLP (H = hemolysis, EL = increased liver enzyme levels in the blood, LP = decreased platelet levels) was introduced by Louis Weinstein, who in 1982 presented the results of an analysis of a group of pregnant women with highly pronounced consequences of preeclampsia and eclampsia [2,6]. The researcher showed that all patients had hemolytic anemia associated with microangiopathy, changes in the shape of erythrocytes in the peripheral smear, moderate to severe thrombocytopenia, and abnormal enzymatic tests of liver function, usually in combination with epigastric pain, nausea and vomiting, and severe hypertension and proteinuria often coexisted with these symptoms [3,6]. Since the publication of L. Weinstein's work, others have made significant research contributions to understanding the pathogenesis, natural history, clinical spectrum, classification, and management strategies for this syndrome [3].<br />HELLP syndrome typically develops suddenly in the 2nd or 3rd trimester of pregnancy or within 48 hours of delivery [5,7,8]. It usually accompanies preeclampsia/eclampsia, but can also occur independently. As in the aforementioned conditions, the likely cause of the syndrome is abnormal placental development and ischemia, which induce oxidative stress, resulting in the release of factors that systematically damage the vascular endothelium through platelet activation, vasoconstriction, and loss of the typical pregnancy-related relaxation of vascular smooth muscle [3,9-13].<br />The liver plays a central role in the pathogenesis of HELLP syndrome and is key to understanding the nature of the disorder. Dysfunction and death of perihepatic hepatocytes in a given patient likely correlates with the severity of the condition. The previously discovered CD95 protein (APO-1, FAS), which plays an important role in the pathogenesis of liver disease, mediates hepatocyte apoptosis by binding to Fas-ligand protein (a ligand for the Fas receptor), a member of the TNF receptor family. Fas-ligand is produced by the placenta, and its serum levels increase during the course of the disease and correlate with its severity. Blocking CD95 signaling reduces serum hepatocytotoxic activity in HELLP syndrome [15].<br />This model of HELLP syndrome pathophysiology has been confirmed by other studies, demonstrating that the liver is the target and the placenta is the initiator of the disorders [3].<br />Many authors emphasize the similarity of HELLP syndrome to the Systemic Inflammatory Response Syndrome (SIRS), which may be evidenced by high levels of inflammatory mediators in serum and liver tissues and clinically available laboratory parameters such as the level of leukocytosis, which increases proportionally to the advancement of the disease [15-17].<br />Currently, there are two basic laboratory classification systems for HELLP syndrome: Mississippi and Tennessee, which were created for the purposes of diagnosis, assessment of disease advancement, and evaluation of treatment efficacy [2,3]. Considered separately, they also provide a platform for comparison of research results. They were developed in the 1980s at the research centers of the Universities of Tennessee and Mississippi.<br />The Mississippi classification takes into account the values of three basic parameters measured in blood serum: platelets, liver enzymes - AST and ALAT, and lactate dehydrogenase - LDH, which correlates with the intensity of hemolysis. Classification is ultimately determined by the lowest platelet count in the course of the disease. Grade 1 is associated with the most severe form of the disease, and grade 3 with the mildest. In this classification, all three parameters must be abnormal to diagnose HELLP syndrome.<br /><br />Mississippi Classification:<br />1. Platelet count 50,000, AST and/or ALAT 70 IU/L, LDH 600 IU/L<br />2. Platelet count 100,000, AST and/or ALAT 70 IU/L, LDH 600 IU/L<br />3. Platelet count 150,000, AST and/or ALAT 40 IU/L, LDH 600 IU/L<br /><br />The second classification system that has become common is the Tennessee classification. It defines the so-called true (complete) and incomplete (partial) HELLP syndrome.<br /><br />Tennessee classification:<br />1. Complete HELLP syndrome: platelet count 100,000, AST 70 IU/L; LDH 600 IU/L or bilirubin 1.2 mg/% and abnormal erythrocyte count
Zaburzenia erekcji w chorobach somatycznych
Erectile dysfunction in somatic diseases
Internal MedicineAs defined, erectile dysfunction (ED, erectile dysfunction) is the persistent inability to achieve and/or maintain an erection sufficient for satisfactory sexual activity (symptoms must persist for a minimum of three months, unless ED is associated with trauma or surgery surgery). It is estimated that 3 million men in Poland are affected, and in a population with cardiovascular disease (CVD, or Cardiovascular Disease) it affects nearly 80% of patients.
Zastosowanie lipegfilgrastymu w pierwotnej profilaktyce gorączki neutropenicznej w trakcie chemioterapii dosedense u pacjentki z rakiem piersi — opis przypadku
Administration of lipegfilgrastim in primary prophylaxis of febrile neutropenia during dose-dense chemotherapy in a patient with breast cancer — case report
Internal MedicineThe use of dose-dense or "dense-dose" complementary chemotherapy in early breast cancer has allowed significantly improve the four-year disease-free survival (DFS) rate, especially in a group of patients who are young and have the so-called triple-negative (tripple negave) breast cancer phenotype. This mode of administration of chemotherapy is associated with a significantly higher (about 20%) risk of neutropenic fever (GN). As part of primary prophylaxis, current standards use granulocyte colony-stimulating agents granulocyte colony-stimulating agents, mainly the long-acting form - pegfilgrastim. Recently, a new long-acting G-CSF - lipegfilgrastim.
Zarys problemu chorób rzadkich na podstawie omówienia serii przypadków pacjentów z chorobą Gauchera
An outline of the problem of rare diseases based on the presentation of case series of patients with Gaucher disease
Internal MedicineRare disease affects less than 1 person/2000 population. To date, 6,000 rare diseases have been detected. Each person is a carrier of 5-10 genes for rare diseases (mostly recessive genes). The rarity of of these diseases usually leads to a delay in making a correct diagnosis, sometimes by many years.

Wspólne podłoże immunogenetyczne zapalenia części płaskiej ciała rzęskowego i stwardnienia rozsianego — opis przypadku
Common immunogenic background of pars planitis and multiple sclerosis — a case report
Internal MedicineMultiple sclerosis (MS) is the most common central nervous system (CNS) disease of unknown etiologii. There is a hypothesis of an interaction between the major tissue compatibility complex (HLA), activation of lymphocytes T lymphocytes and unknown factors initiating abnormal immune responses. An increased incidence of of uveitis in patients with MS, the most common form of which is inflammation of the part of the flat of the ciliary body (PP).