Publications
Peer-reviewed clinical case reports
Techniki robotyczne i wspomagane laserowo w chirurgii urologicznej: aktualne zastosowania
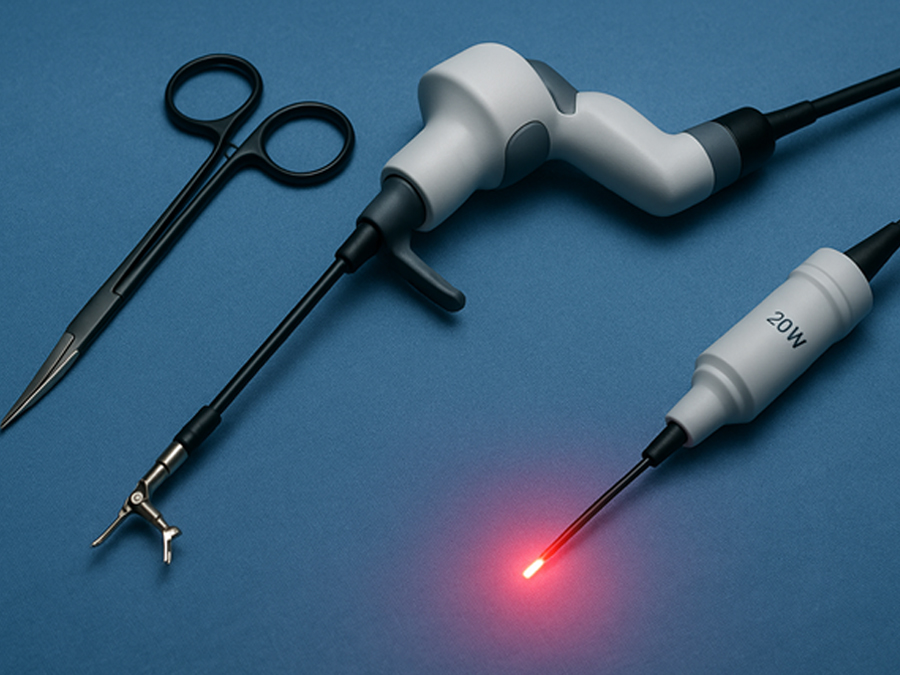
Robotic and Laser-Assisted Techniques in Urologic Surgery: Current Applications
SurgeryMethods This narrative literature review was conducted by systematically searching online databases including PubMed, Scopus, and Cochrane Library for publications between January 2018 and May 2025. The primary focus was on clinical applications of robotic and laser-assisted surgical techniques in urology. The search strategy employed keywords and Boolean operators such as: “robotic surgery” AND “urology”, “laser enucleation” OR “HoLEP” OR “PVP”, “minimally invasive” AND “urologic cancer”, “robot-assisted prostatectomy” OR “robot-assisted nephrectomy”. Inclusion criteria were: • Peer-reviewed studies, clinical trials, meta-analyses, and systematic reviews. • Publications in English. • Studies involving adult patients undergoing urologic procedures. • Focus on either robotic-assisted or laser-assisted interventions. Exclusion criteria were: • Case reports, letters to the editor, or editorials without data. • Non-English publications. • Studies focused exclusively on veterinary or pediatric populations (except where relevant for robotic urology). A total of 137 articles were identified. After screening titles and abstracts, 68 full-text articles were reviewed, and 38 studies were included in this review based on relevance, methodological quality, and recency. The primary endpoints analyzed were operative time, estimated blood loss (EBL), length of hospital stay, complication rates, and functional outcomes. Secondary endpoints included cost analysis, training requirements, and ethical implications. Robotic-Assisted Urologic Procedures Robotic-assisted surgery has revolutionized the field of urology by enhancing precision, minimizing invasiveness, and improving postoperative outcomes. The da Vinci Surgical System, approved by the FDA in 2000, remains the most widely used platform. Robotic platforms enable three-dimensional magnified vision, greater instrument articulation, and improved ergonomics, all of which are critical for complex pelvic and retroperitoneal procedures. Robotic Radical Prostatectomy (RARP) Radical prostatectomy is one of the most established robotic procedures in urology. Robotic-assisted radical prostatectomy (RARP) has largely replaced open and laparoscopic techniques due to superior visualization of the neurovascular bundles and improved continence and erectile function recovery in some cohorts (1). Multiple studies demonstrate comparable oncologic control between RARP and open surgery, with significantly reduced blood loss, lower transfusion rates, and shorter hospitalization(2). Innovations like dual-console systems and nerve-sparing algorithms are further enhancing patient outcomes. Robotic Partial and Radical Nephrectomy Robotic partial nephrectomy (RPN) is considered the standard for small renal masses due to its nephron-sparing advantages. The robotic approach allows precise tumor excision with minimal warm ischemia time and improved suturing of the renal defect(3). Compared to laparoscopic partial nephrectomy, RPN demonstrates lower conversion rates and better postoperative renal function(4)Robotic radical nephrectomy, while less commonly used than partial nephrectomy, is advantageous in selected cases for complex tumor locations or large renal masses.
Nietrzymanie moczu po prostatektomii: czynniki ryzyka, rehabilitacja i opcje chirurgiczne
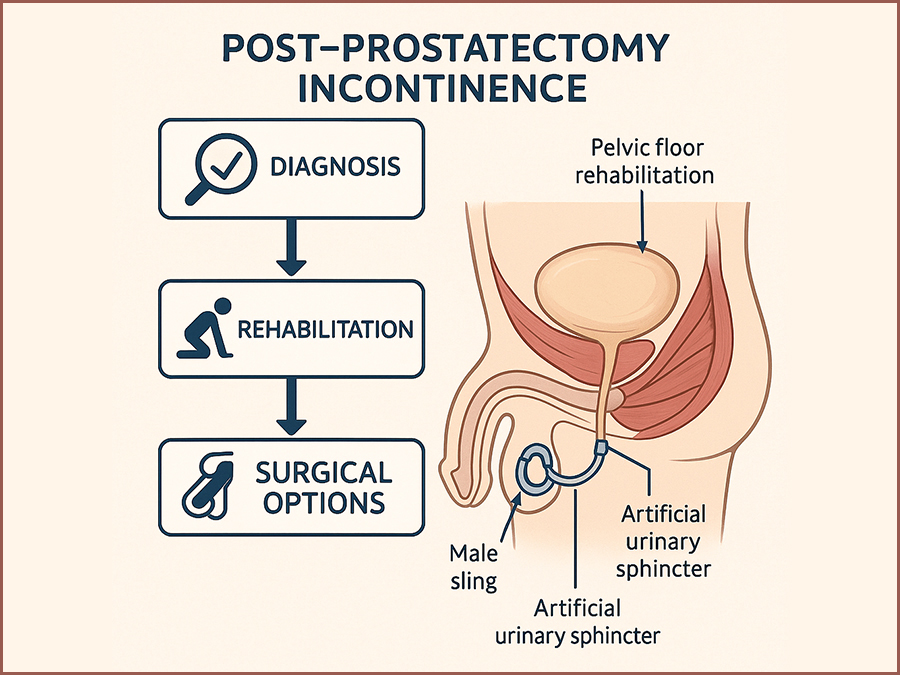
Post-Prostatectomy Incontinence: Risk Factors, Rehabilitation, and Surgical Options
SurgeryRadical prostatectomy is a cornerstone of curative therapy for localized prostate cancer, offering favorable oncologic outcomes in appropriately selected patients. However, one of its most common and distressing complications is post-prostatectomy incontinence (PPI), with reported rates ranging from 4% to 40% depending on the definition used, the surgical technique, and the timing of assessment. (1,2) This complication significantly impacts health-related quality of life, causing physical discomfort, emotional distress, and social withdrawal.(3) PPI differs from other types of male urinary incontinence in both etiology and management. It primarily results from iatrogenic damage to the sphincteric mechanism during prostate removal, although additional contributing factors include detrusor overactivity, impaired compliance, and changes in bladder neck dynamics.(4,5) Despite advancements in minimally invasive and robotic-assisted surgical approaches, PPI remains a challenge for both patients and clinicians. A comprehensive understanding of the pathophysiology and risk factors for PPI is essential to develop optimal prevention and management strategies. In addition, clinicians must be well-versed in both non-surgical and surgical treatment modalities to tailor therapy to individual patient needs and expectations.(6,7) This review aims to synthesize the current evidence on PPI, focusing on identifiable risk factors, effective rehabilitative strategies, and available surgical treatments. By consolidating contemporary research and clinical guidelines, this paper seeks to provide a clear framework for the management of PPI in urologic practice.
Infekcja COVID-19 imitująca ostrą białaczkę promielocytową
COVID-19 infection mimicking acute promyelocytic leukemia
SurgeryAcute promyelocytic leukemia (APL) is a subtype of acute myeloid leukemia (AML) that underlies a block of differentiation at the promyelocyte level, which in 95% of cases is mediated by a translocation between chromosomes 15 and 17, t(15;17)(q22,q21), resulting in a fusion of the PML and RARA genes. As a result, the PML-RARα fusion protein is produced, the presence of which leads to self-renewal and inhibition of cell differentiation from the myeloid lineage at the promyelocyte stage [1, 2]. The disintegrating promyelocytes release thromboplastic granules, resulting in the induction of disseminated intravascular coagulation (DIC) syndrome, with secondary fibrinolysis and a high risk of fatal hemorrhagic complications [3]. The diagnosis of APL is made on the basis of clinical symptoms, results of peripheral blood count, flow cytometry and marrow studies including cytogenetic and molecular tests. The myelogram shows the presence of abnormal morphological promyelocytes containing characteristic granules in the cytoplasm, the so-called Aurea scabra. On cytometric examination, the analyzed marrow cells are characterized by high expression of CD13, CD33 antigens and low or absent expression of CD11b, CD34, CD117, HLA-DR antigens. However, in order to diagnose APL, it is necessary to demonstrate the presence of t(15;17) translocation by FISH or PML-RARα protein by RT-PCR or other common, less common RARα gene rearrangements [1, 4]. Due to the high risk of developing DIC syndrome and the associated high risk of patient death, antitumor treatment is already initiated when APL is suspected, that is, before results confirming the t(15;17) translocation and/or PML-RARα gene rearrangement are obtained. Treatment is based on the use of all-trans retinoic acid (ATRA), which affects the conformation of the abnormal PML-RARα fusion protein, resulting in the induction of differentiation and maturation of promyelocytes [1, 5]. COVID-19 infection is still a poorly understood disease entity. The course of the infection, its complications and distant effects are not fully known. In some cases, it may be suspected of contributing to hematopoietic dysfunction, resulting in impaired maturation of various cell lines. Covid-19 infection can, among other things, lead to the proliferation of blastic cells in the blood or bone marrow, even suggesting a diagnosis of acute proliferative disease [6]. We present the case of a patient who developed hematologic abnormalities mimicking acute promyelocytic leukemia during COVID-19 infection.
Zastosowanie technologii water i koagulacji plazmą argonową w chirurgii organooszczędzającej guza nerki – opis przypadku
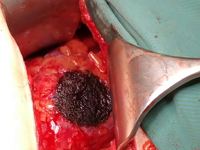
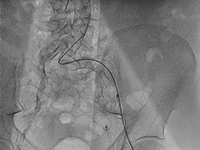
Application of water jet technology and argon plasma coagulation in nephron-sparing surgery for a kidney tumour – a case report.
SurgeryOwing to the ever increasing role of medical imaging (e.g. ultrasonography, computed tomography or magnetic resonance imaging), the number of incidentally detected kidney tumours is growing as well. These tumours are usually small renal masses (SRMs) at early advancement stages (1). According to the guidelines of the European Society of Urology, kidney tumours at early stages (T1) should be treated with nephron-sparing surgery (NSS). In the long term, this type of treatment allows renal function preservation, decreases overall mortality and reduces the incidence of cardiovascular events (2). The main goals of NSS are tumour removal with negative surgical margins and preservation of the best possible function of the remaining renal parenchyma with minimised risk of adverse events. The progress of medical technologies renders surgical procedures more and more effective.

Zespół Wunderlicha objawiający się samoistnym krwotokiem nerkowym w jamie zaotrzewnowej jako pierwsza manifestacja raka nerkowokomórkowego
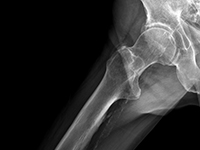
Wunderlich Syndrome presenting as Spontaneous renal haemorrhage in the retroperitoneal cavity as the first manifestation of renal cell carcinoma.
SurgerySpontaneous, nontraumatic retroperitoneal hemorrhage or Wunderlich syndrome (WS) is a rare but potential life-threatening condition. It can prove fatal if not recognized and treated aggressively at the appropriate time. A shock caused by massive retroperitoneal or intraperitoneal haemorrhage may develop in isolated cases [1]. The clinical findings are not specific, which is why the differential diagnosis must be made with a multitude of benign and malignant renal masses until the correct diagnosis can be made by the pathologist. The CT and US images are not characteristic. The most common cause of bleeding is angiomiolipoma. Less often are drug-induced vasculitis, kidney cancer, pheochromocytoma or renal cyst. We present the case of 53-year old man with symptoms of renal haemorrhage in the retroperitoneal cavity as the first manifestation of renal cell carcinoma.

Możliwości leczenia systemowego u chorych na NDRP po przeszczepie narządów - opis przypadku i przegląd literatury
Possibilities of systemic treatment in patients with NSCLC after organ transplantation - case report and literature review
SurgeryThe introduction of antibiotics, mass vaccinations to prevent infectious diseases and organ transplants can be considered the greatest achievements of 20th century medicine. Solid organ transplants save the lives of patients suffering from organ failure and improve their quality of life. The life expectancy of transplant patients has improved significantly over the past two decades. Successful transplantation improves survival in patients on chronic dialysis and in patients with irreversible liver, heart and lung disease and end-stage failure of these organs. The percentage of transplants performed is steadily increasing, but is still insufficient [1]. According to data reported to the Global Observatory on Donation and Transplantation (GODT), 106,879 organ transplants were performed in 95 countries worldwide in 2010, including:73,179 kidney transplants (46% from living donors), 21,602 liver transplants (15% from living donors), 5582 heart transplants, 3927 lung transplants, 2362 pancreas transplants and 227 small bowel transplants. This activity increased by 2.12% compared to 2009 [2].Unfortunately, it is estimated that the number of transplants performed is insufficient. At the same time, there are huge geographic differences in the number of transplants per million population: from 70 per million population in developed countries to 0-2.4 in developing countries [3]. As transplantation prolongs patients' lives, cancers are becoming an increasing threat to long-term survival, especially in patients who have undergone liver transplantation for hepatocellular carcinoma (HCC)[4].The risk of cancer in transplant patients is higher than in the general population. This is due to three reasons. Immunosuppressive treatment accompanying organ transplantation causes a decline in immunity, which can promote infection with oncogenic viruses such as humanpapillomavirus (HPV) or humanherpesvirustype 8 (HHV-8), and can allow emerging cancer cells to escape from weakened immune surveillance. In addition, immunosuppressive drugs have a cytotoxic effect, which can induce the formation of mutations and the transformation of normal cells into cancer cells. Therefore, patients undergoing organ transplantation most often develop hemato-oncologic malignancies, cancers associated with infection with potentially oncogenic viruses: Kaposi's sarcoma (infection with human herpes viruses), cervical cancer and squamous cell carcinomas of the head and neck region (infection with human papillomavirus), liver cancer (infection with hepatitis B and C viruses) and skin cancers. Lung cancer, cancers of the gastrointestinal tract or urinary tract occur in no more than 1% of transplant recipients. The feasibility of using systemic cancer treatment in organ transplant patients has yet to be explored. The most controversial is the use of immunotherapy in cancer patients previously undergoing organ transplantation and immunosuppressive treatment. Modern cancer immunotherapies targeting immune checkpoints are designed to enhance the immune response, and thus may increase the risk of transplant rejection. Lung cancer is one of the leading causes of death from malignant tumors worldwide. There are two main types of lung cancer: non-small cell lung cancer (NDRP) and small cell lung cancer (DRP). NDRP is much more common, accounting for 80-85% of lung cancer cases. Thoracic surgery, chemotherapy and radiation therapy have been used to treat lung cancer [5]. Due to unsatisfactory treatment results, the search for new therapies began. The use of immunotherapy and molecularly targeted therapies proved to be a breakthrough. These therapies have been successfully used in selected patients with locally advanced and metastatic NDRP. These therapies have led to an increase in disease progression-free time and overall survival of patients, allowing lung cancer to be classified as a chronic disease [6].

Czy zawsze udaje się ustalić etiologię ostrego zapalenia trzustki? Rzadki przypadek kliniczny OZT u chorej z erytromelalgią pierwotną
Can the etiology of acute pancreatitis always be identified? A rare case of acute pancreatitis in a patient with primary erythromelalgia
SurgeryAPD is the most common pancreatic disease and also a quite frequent cause of hospitalization of patients presenting to the hospital for due to abdominal pain. There has been an increasing incidence in recent years in developed countries and mortality in this disease reaching 5%. [1, 2]. Accurate diagnostics should make it possible to determine the etiology of UTI in more than 96% of cases [3] this, however, is still not achieved in many patients this is not achieved. Thus, relapse may occur with reoccurrence of a previously unrecognized etiologic factor. Many authors raise the role of drugs as a potential causative factor of ICS of unclear etiology[4]. There is no strictly defined regimen for effective yet safe treatment of pain in ICS. To date, it has not been established to what extent the drugs used for pain relief in this disease may simultaneously be a causative factor in pancreatitis[5, 6]. Primary erythromelalgia (EM), is a rare, genetically determined disease manifested by pain in the extremities, their increased heat and redness [7] [Image 1 - Painful erythema of the extremities lower extremities is the most common symptom in patients with Primary Erythromelalgia]. Treatment pharmacological treatment of this disease is not always effective. Various physical and invasive methods, including neurolysis of the lumbar segment of the sympathetic trunk sympathetic trunk [8]. This causes patients with EM often overuse pain medications, some of which are also used in the symptomatic treatment of pain in EM. We present the case of a 25- year-old EM patient who developed symptoms of ICS 10 days after unsuccessful pharmacological neurolysis of the lumbar sympathetic trunk and was preceded by the use of several analgesics, later also used in the treatment of during treatment of pancreatitis. Despite thorough diagnostics, it was not possible to determine the cause of the OST
Pacjent z wielonaczyniową chorobą wieńcową i schyłkową niewydolnością nerek leczony wielokrotnymi przezskórnymi interwencjami wieńcowymi.
Patient with multivessel coronary artery disease and end-stage renal disease treated with multiple percutaneous coronary interventions.
SurgeryEnd-stage renal failure (SNN) is a growing problem in developed countries [1]. Although diabetes remains the most common cause of dysfunction of these organs [2], chronic nephropathy can also be caused by autoimmune diseases, particularly from the vasculitis group. In the United States, the number of patients with SNN requiring dialysis therapy already reaches nearly 500,000, and more than 200,000 are living with an active kidney transplant [3]. Chronic kidney disease (CHD) is a significant cardiovascular problem, contributing to the rapid development of coronary artery disease coronary artery disease, especially the multivessel form. The more severe course of coronary artery disease coronary artery disease in patients with PChN is influenced by impaired calcium metabolism and a tendency to diffuse arterial calcification [4]. Patients with PChN and high CRP levels are at particularly high risk of cardiovascular incidents [5,6]. Currently, there are no guidelines for the surgical treatment of coronary artery disease in patients with PChN. However, they have a higher risk of death after revascularization than in the population without PChN [7]. Opinions on the effectiveness of of using percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) are divided, and there are no conclusive data in this regard. There are also no recommendations suggesting the development of a long-term strategy for treating coronary artery disease in patients with SNN, although it has been it has been described that they require multiple repeat PCI (if this method is chosen method) [8].

Nawrót przepukliny przeponowej u 21 letniego mężczyzny – opis przypadku.
Recurrence of diaphragmatic hernia in a 21-year-old man - case report.
SurgeryCongenital diaphragmaƟc hernia (CDH) is a developmental defect consisƟng in the dislocaƟon of abdominal organs into the chest. The displacement occurs through a hole in the diaphragm formed during the fetal period. The recurrence of diaphragmaƟc hernia is rare and appeared most oŌen aŌer a few weeks aŌer surgery.
Rak nerki związany z nabytą torbielowatością nerek - nowa jednostka w klasyfikacji WHO 2016. Opis dwóch przypadków wykrytych na wczesnym etapie rozwoju.
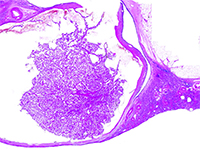
Acquired cystic disease associated renal cell carcinoma - new entity in classification WHO 2016. Report of two cases detected at an early stage of development.
SurgeryW 2012 roku The International Society of Urological Pathology (ISUP) zaproponowało wdrożenie do klasyfikacji 5 nowych podtypów raka nerki, w tym raka nerki związanego z nabytą torbielowatością nerek (ang. acquired cystic disease - associated renal cell carcinoma - ACD-RCC). W 2016 roku ACD-RCC został uznany za niezależną jednostkę w Klasyfikacji Nowotworów Układu Moczowego WHO 2016. [1]. Poniższa praca prezentuje typowe cechy ACD-RCC w oparciu o dwa przypadki.
Nawrót pierwotnie niezdiagnozowanej polimialgii reumatycznej (PMR) po 6 latach od wystąpienia pierwszych objawów
The recurrence of an originally undiagnosed polymyalgia rheumatica (PMR) 6 years after its first symptoms occurrence
SurgeryPolymyalgia rheumatica (PMR) is one of the most common rheumatic diseases diagnosed in people over 50 years of age. Its incidence increases with age, reaching a peak at 72-73 years of age (PMR is rarely diagnosed in the 50-year-old population) [1]. Statistically, it affects women twice as often. A greater predisposition is also observed in the white race [2]. In Europe, the incidence is on average 1 in 133 people over 50 years of age [3]. There is also a clear geographical variation – the vast majority of diagnoses occur in Northern European countries, particularly Sweden, while in Southern Europe, for example, in Italy, it is much less frequently diagnosed. The etiology of the disease has not been fully elucidated. It is assumed that autoimmune processes underlie it. The role of solar radiation and viral infections has also been suggested [2]. Typical symptoms of polymyalgia include pain and stiffness in the neck, shoulder girdle, and hip muscles [1,2]. PMR belongs to a group of inflammatory diseases with an immune basis. Its etiology also includes a genetic predisposition, including the involvement of antigens: HLA-DR4, HLADRB1*04, and proinflammatory cytokines: TNFα and IL6. Some studies have also demonstrated reduced secretion of adrenal cortex hormones (cortisol, dehydroepiandrosterone) in individuals affected by this condition [4]. The variety of factors postulated to play a significant role in the development of PMR indicates the need for further research into the etiology of this disease.

Przypadkowo wykryty rak języka u pacjenta z niedokrwistością i bólami stawów.
Tongue cancer diagnosed incidentally in a patient with anaemia and joint pain.
SurgeryTongue cancer is the most common oral cancer [1]. Most patients report exposure to known risk factors for cancer development, such as frequent alcohol consumption, smoking, and poor oral hygiene [1, 2]. Unfortunately, due to the tumor's location and patients' failure to appreciate early symptoms, most diagnoses are made in very advanced stages of the disease [2]. We present a case report of a patient with incidentally diagnosed tongue cancer.