Publications
Peer-reviewed clinical case reports
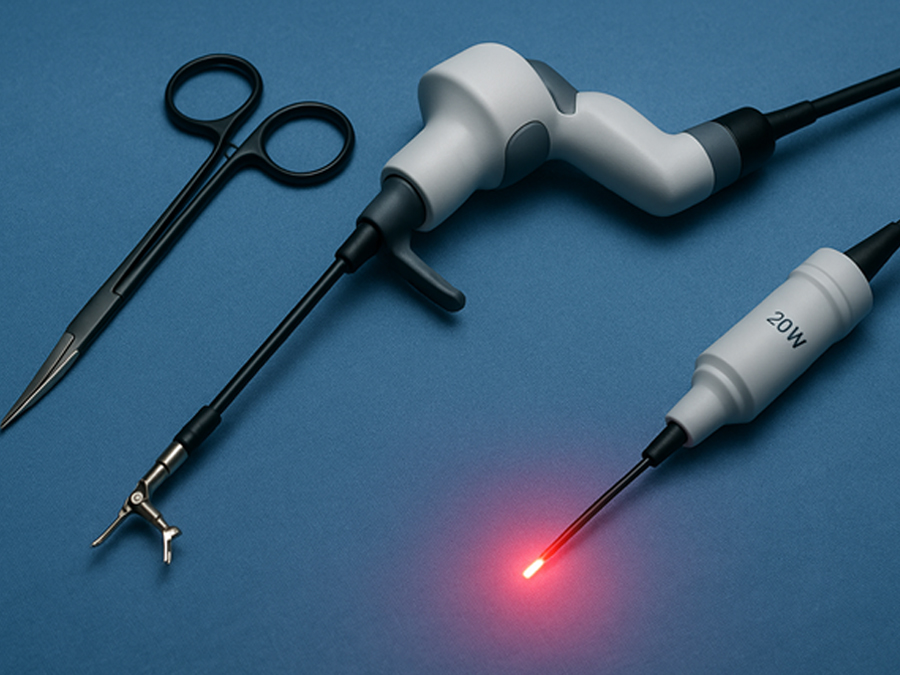
Techniki robotyczne i wspomagane laserowo w chirurgii urologicznej: aktualne zastosowania
Robotic and Laser-Assisted Techniques in Urologic Surgery: Current Applications
SurgeryMethods This narrative literature review was conducted by systematically searching online databases including PubMed, Scopus, and Cochrane Library for publications between January 2018 and May 2025. The primary focus was on clinical applications of robotic and laser-assisted surgical techniques in urology. The search strategy employed keywords and Boolean operators such as: “robotic surgery” AND “urology”, “laser enucleation” OR “HoLEP” OR “PVP”, “minimally invasive” AND “urologic cancer”, “robot-assisted prostatectomy” OR “robot-assisted nephrectomy”. Inclusion criteria were: • Peer-reviewed studies, clinical trials, meta-analyses, and systematic reviews. • Publications in English. • Studies involving adult patients undergoing urologic procedures. • Focus on either robotic-assisted or laser-assisted interventions. Exclusion criteria were: • Case reports, letters to the editor, or editorials without data. • Non-English publications. • Studies focused exclusively on veterinary or pediatric populations (except where relevant for robotic urology). A total of 137 articles were identified. After screening titles and abstracts, 68 full-text articles were reviewed, and 38 studies were included in this review based on relevance, methodological quality, and recency. The primary endpoints analyzed were operative time, estimated blood loss (EBL), length of hospital stay, complication rates, and functional outcomes. Secondary endpoints included cost analysis, training requirements, and ethical implications. Robotic-Assisted Urologic Procedures Robotic-assisted surgery has revolutionized the field of urology by enhancing precision, minimizing invasiveness, and improving postoperative outcomes. The da Vinci Surgical System, approved by the FDA in 2000, remains the most widely used platform. Robotic platforms enable three-dimensional magnified vision, greater instrument articulation, and improved ergonomics, all of which are critical for complex pelvic and retroperitoneal procedures. Robotic Radical Prostatectomy (RARP) Radical prostatectomy is one of the most established robotic procedures in urology. Robotic-assisted radical prostatectomy (RARP) has largely replaced open and laparoscopic techniques due to superior visualization of the neurovascular bundles and improved continence and erectile function recovery in some cohorts (1). Multiple studies demonstrate comparable oncologic control between RARP and open surgery, with significantly reduced blood loss, lower transfusion rates, and shorter hospitalization(2). Innovations like dual-console systems and nerve-sparing algorithms are further enhancing patient outcomes. Robotic Partial and Radical Nephrectomy Robotic partial nephrectomy (RPN) is considered the standard for small renal masses due to its nephron-sparing advantages. The robotic approach allows precise tumor excision with minimal warm ischemia time and improved suturing of the renal defect(3). Compared to laparoscopic partial nephrectomy, RPN demonstrates lower conversion rates and better postoperative renal function(4)Robotic radical nephrectomy, while less commonly used than partial nephrectomy, is advantageous in selected cases for complex tumor locations or large renal masses.
Nietrzymanie moczu po prostatektomii: czynniki ryzyka, rehabilitacja i opcje chirurgiczne
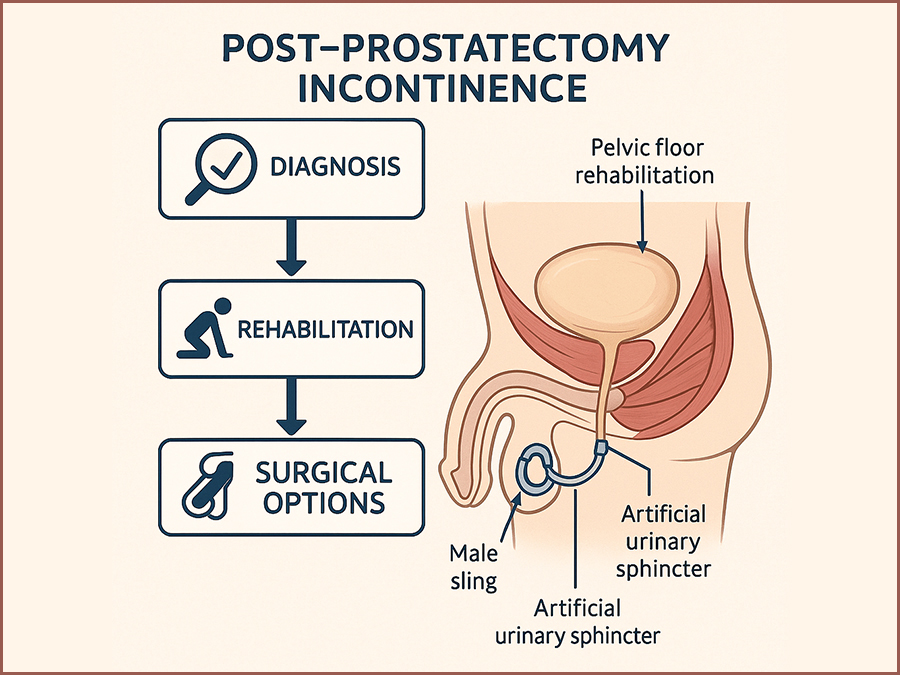
Post-Prostatectomy Incontinence: Risk Factors, Rehabilitation, and Surgical Options
SurgeryRadical prostatectomy is a cornerstone of curative therapy for localized prostate cancer, offering favorable oncologic outcomes in appropriately selected patients. However, one of its most common and distressing complications is post-prostatectomy incontinence (PPI), with reported rates ranging from 4% to 40% depending on the definition used, the surgical technique, and the timing of assessment. (1,2) This complication significantly impacts health-related quality of life, causing physical discomfort, emotional distress, and social withdrawal.(3) PPI differs from other types of male urinary incontinence in both etiology and management. It primarily results from iatrogenic damage to the sphincteric mechanism during prostate removal, although additional contributing factors include detrusor overactivity, impaired compliance, and changes in bladder neck dynamics.(4,5) Despite advancements in minimally invasive and robotic-assisted surgical approaches, PPI remains a challenge for both patients and clinicians. A comprehensive understanding of the pathophysiology and risk factors for PPI is essential to develop optimal prevention and management strategies. In addition, clinicians must be well-versed in both non-surgical and surgical treatment modalities to tailor therapy to individual patient needs and expectations.(6,7) This review aims to synthesize the current evidence on PPI, focusing on identifiable risk factors, effective rehabilitative strategies, and available surgical treatments. By consolidating contemporary research and clinical guidelines, this paper seeks to provide a clear framework for the management of PPI in urologic practice.
Infekcja COVID-19 imitująca ostrą białaczkę promielocytową
COVID-19 infection mimicking acute promyelocytic leukemia
SurgeryAcute promyelocytic leukemia (APL) is a subtype of acute myeloid leukemia (AML) that underlies a block of differentiation at the promyelocyte level, which in 95% of cases is mediated by a translocation between chromosomes 15 and 17, t(15;17)(q22,q21), resulting in a fusion of the PML and RARA genes. As a result, the PML-RARα fusion protein is produced, the presence of which leads to self-renewal and inhibition of cell differentiation from the myeloid lineage at the promyelocyte stage [1, 2]. The disintegrating promyelocytes release thromboplastic granules, resulting in the induction of disseminated intravascular coagulation (DIC) syndrome, with secondary fibrinolysis and a high risk of fatal hemorrhagic complications [3]. The diagnosis of APL is made on the basis of clinical symptoms, results of peripheral blood count, flow cytometry and marrow studies including cytogenetic and molecular tests. The myelogram shows the presence of abnormal morphological promyelocytes containing characteristic granules in the cytoplasm, the so-called Aurea scabra. On cytometric examination, the analyzed marrow cells are characterized by high expression of CD13, CD33 antigens and low or absent expression of CD11b, CD34, CD117, HLA-DR antigens. However, in order to diagnose APL, it is necessary to demonstrate the presence of t(15;17) translocation by FISH or PML-RARα protein by RT-PCR or other common, less common RARα gene rearrangements [1, 4]. Due to the high risk of developing DIC syndrome and the associated high risk of patient death, antitumor treatment is already initiated when APL is suspected, that is, before results confirming the t(15;17) translocation and/or PML-RARα gene rearrangement are obtained. Treatment is based on the use of all-trans retinoic acid (ATRA), which affects the conformation of the abnormal PML-RARα fusion protein, resulting in the induction of differentiation and maturation of promyelocytes [1, 5]. COVID-19 infection is still a poorly understood disease entity. The course of the infection, its complications and distant effects are not fully known. In some cases, it may be suspected of contributing to hematopoietic dysfunction, resulting in impaired maturation of various cell lines. Covid-19 infection can, among other things, lead to the proliferation of blastic cells in the blood or bone marrow, even suggesting a diagnosis of acute proliferative disease [6]. We present the case of a patient who developed hematologic abnormalities mimicking acute promyelocytic leukemia during COVID-19 infection.

Postępowanie w dystocji barkowej u pacjentki rodzącej do wody - studium przypadku
The management in shoulder dystocia during water birth- case study.
GynecologyThis study describes a management of shoulder dystocia during water birth. It contains a guideline for the management of shoulder dystocia developed by the Obstetrics and Gynecology Ward and Chair in Tychy.
Zastosowanie technologii water i koagulacji plazmą argonową w chirurgii organooszczędzającej guza nerki – opis przypadku
Application of water jet technology and argon plasma coagulation in nephron-sparing surgery for a kidney tumour – a case report.
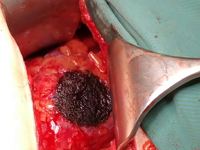
SurgeryOwing to the ever increasing role of medical imaging (e.g. ultrasonography, computed tomography or magnetic resonance imaging), the number of incidentally detected kidney tumours is growing as well. These tumours are usually small renal masses (SRMs) at early advancement stages (1). According to the guidelines of the European Society of Urology, kidney tumours at early stages (T1) should be treated with nephron-sparing surgery (NSS). In the long term, this type of treatment allows renal function preservation, decreases overall mortality and reduces the incidence of cardiovascular events (2). The main goals of NSS are tumour removal with negative surgical margins and preservation of the best possible function of the remaining renal parenchyma with minimised risk of adverse events. The progress of medical technologies renders surgical procedures more and more effective.

Zespół Wunderlicha objawiający się samoistnym krwotokiem nerkowym w jamie zaotrzewnowej jako pierwsza manifestacja raka nerkowokomórkowego
Wunderlich Syndrome presenting as Spontaneous renal haemorrhage in the retroperitoneal cavity as the first manifestation of renal cell carcinoma.
SurgerySpontaneous, nontraumatic retroperitoneal hemorrhage or Wunderlich syndrome (WS) is a rare but potential life-threatening condition. It can prove fatal if not recognized and treated aggressively at the appropriate time. A shock caused by massive retroperitoneal or intraperitoneal haemorrhage may develop in isolated cases [1]. The clinical findings are not specific, which is why the differential diagnosis must be made with a multitude of benign and malignant renal masses until the correct diagnosis can be made by the pathologist. The CT and US images are not characteristic. The most common cause of bleeding is angiomiolipoma. Less often are drug-induced vasculitis, kidney cancer, pheochromocytoma or renal cyst. We present the case of 53-year old man with symptoms of renal haemorrhage in the retroperitoneal cavity as the first manifestation of renal cell carcinoma.

Izolowany nerwiakowłókniak splotowy ręki: opis dwóch przypadków. Propozycje diagnostyki i leczenia.
Isolated hand plexus neurofibroma: two case reports. Diagnostics and treatment proposals.
GynecologyNeurofibromas Plexiform neurofibromas are benign tumors of the peripheral nerve sheath. They can be found as single or multiple nodules, which are part of the of the clinical picture in any type of neurofibromatosis, and can become malignant. Neurofibromas arise from Schwann cells which are part of the nerves of the skin throughout the body, nerves innervating internal organs and cranial nerves. The most characteristic symptoms include the presence of scattered, elongated, resilient subcutaneous nodules. These are fibromas, histologically resembling individual neurofibromas, appearing along the the course of peripheral nerves or cranial nerves. They most often occur on the face and neck. Sometimes they lead to massive enlargement of a limb or other part of the body (neurofibromatous elephantiasis) [1,2]. Another equally common common symptom is skin discoloration, looking resembling coffee spots ("giant café-au-lait spot"), as well as freckle-like lesions localized around the axillae and axillary pits [3]. Neurological symptoms are associated with the compression of neurofibromas on adjacent structures. The patient then complains of neuralgia of the peripheral nerves. In the literature we can find isolated cases of neurofibroma plexiformis without any association with neurofibromatosis type 1 [4-6]. Treatment of patients with plexiform neurofibromas is not well defined defined and is mainly aimed at controlling symptoms. Surgical excision is the only available therapy, as there there are no drugs that can prevent their formation or treat them conservatively conservatively. At present, the results of surgical excision are not fully satisfactory, and these procedures can be complicated due to the size, location, condition of the vessels, involvement of the neural involvement, microscopic staging and high rates of tumor re-growth [7]. It should also take into account the fact that there are known there are many causes causing tumor-like lesions to neurofibromas . These include traumatic soft tissue injuries, arthritis, tendon diseases (e.g. tendinosis, tendon sheath inflammation, tendon rupture), non-neoplastic soft tissue lesions (e.g. ganglion, bursitis, granuloma) , and, less commonly, tumors and their metastases to soft tissues [8]. Focal lesions of soft tissues soft tissues are often the cause of pain and palpable tumor mass [9]. W these cases, especially in the early stages, accurate diagnosis is crucial, to establish a diagnosis and treatment strategy. Therefore, w when confronted with a focal tumor lesion the logical seems is to follow established algorithm of procedure. First, it should provide an accurate description of the lesion in correlation with the patient's age, location, type of involved tissue, the condition of the adjacent environment. For this purpose, in addition to detailed clinical examination, ultrasound should be performed of the occupied area, and if a bony lesion is suspected then an x-ray examination in two projections with adjacent joints. The advancement of bone lesions, it is necessary to deepening diagnosis through CT examination. However, lesion limited only to soft tissues on ultrasound will require MRI diagnosis, which will more accurately visualize the infiltration by its neighborhood. If imaging studies show a high probability of proliferative disease, an important diagnostic element is to obtain material for pathomorphologic examination, taken during open biopsy or oligobiopsy and establish the histological diagnosis [10]. If the neoplastic process is confirmed, it is always necessary to X-ray/CT scan of the chest, ultrasound/CT scan of the abdomen and even even PET to exclude metastases [11]. The second stage of the implemented algorithm dictates that treatment should be planned based on the answers to the following questions: - Is the lesion likely to be a normal variant, i.e., "leave me alone, don't touch me." lesion of a benign type, requiring no further imaging or supplies, but only observation? [12] - Does the lesion have features suggestive of an aggressive nature, and then how far advanced should be treatment? [13]. The heterogeneity of the clinical picture of unidentified focal nodular lesions in the metacarpal region, the variety of available methods of diagnosis do not make the task any easier the task, both at the stage of making the initial diagnosis and during communication between members of the interdisciplinary team, who, on more than one occasion, should handle the treatment. Therefore, it seems important to cooperate on the line of orthopedist-oncologist-pathomorphologist. Two cases of isolated neurofibromatosis of the palm of the hand are described below because of their uniqueness. The second of the described cases indicated an additional possibility of postoperative treatment of the patient in the form of prolotherapy injections to improve the function of the treated limb.

Wybrane odrębności w żywieniu dzieci w trakcie leczenia onkologicznego. Cykl: Leczenie żywieniowe — ab ovo.
Selected differences in nutrition of children during oncological treatment. Nutrition therapy - editorial cycle.
OtherOncological treatment is associated with a high risk of malnutrition in children. Complications of treatment often prevent oral intake of food, which requires proper dietary modification and consideration of parenteral nutrition.
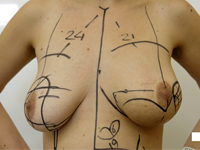
Mastektomia i jednoczasowa rekonstrukcja piersi u chorej na mięsaka gruczołu po przebytym skojarzonym leczeniu oszczędzającym z powodu raka
Mastectomy and immediate reconstruction at woman with breast sarcoma following breast connserving treatment due to cancer
GynecologyBreast sarcomas are rare, accounting for 1% of malignant gland tumors and less than 5% of all tumors mesenchymal neoplasms.1 The low incidence makes it difficult to conduct trials randomized clinical trials, and available data include descriptions of retrospective series and single cases. The number of known factors that increase risk of developing the disease is small. A genetic predisposition in the form of syndrome Li-Fraumeni (TP53 gene mutation) increases the risk of primary sarcomas also in the thoracic location.2 Chronic lymphedema occurring in some patients after axillary lymphadenectomy and axillary irradiation predisposes to lymphangiosarcoma in the affected arm (Stewart syndrome and Treves syndrome).3 Secondary sarcomas occasionally occur in breasts previously irradiated after breast conserving treatment (BCT), performed for breast cancer, the most common malignancy in women, and after radiation therapy administered for malignant granuloma.4 The cumulative risk of of radiotherapy-induced sarcoma (RIS) is 3.2 per 1,000 over 15 years vs. compared to 2.3 per 1,000 for primary sarcoma in a population without radiation therapy.5 Compared to women who were not irradiated, patients treated with radiation therapy for breast cancer, the risk of developing radiotherapy-induced hemangiosarcoma (radiotherapy-induced angiosarcoma, RIA) is five times higher 6 , in general, however, the possibility of of developing angiosarcoma after radiation therapy is low and, according to the literature literature, it is 0.03 - 0.2% in more than 10 years of follow-up.7,8 It should be clearly emphasized the benefits enjoyed by women with breast cancer due to radiation, an obligatory part of breast-saving treatment.9 There has been no correlation of the incidence of RIS with the use of chemotherapy.10 For the The diagnosis of radiotherapy-induced sarcoma can be made using criteria proposed by Cahan in 1948,11 as interpreted by Kirova15 (At that time, Cahan described more than a dozen cases of bone sarcomas in patients irradiated according to the treatment standards of the time for benign lesions and bone tuberculosis, the first point in the original description was the non-neoplastic nature of the lesion treated with radiation therapy)11: 1. History of treatment with irradiation 2. asymptomatic latency period between two cancers lasting several years 3. occurrence of sarcoma in a previously irradiated area, 4. Histopathologic confirmation of sarcoma as a second neoplasm.10,11,15 However Cahan described the latency period as "relatively long," amounting to more than 5 years in his paper, the literature a case has been described that appeared before a year, also described as a RIS (RIA).12 Among the histopathological types diagnosed among secondary sarcomas include angiosarcoma, hemangiosarcoma, leiomyosarcoma, malignant fibrous histiocytoma, liposarcoma, and fibrosarcoma. Also described were chondrosarcoma and osteosarcoma. RIS develop most often in the chest wall, less often in the parenchyma of the of the irradiated breast.10 The method of choice for patients with for breast sarcomas is excision of the tumor with a margin of healthy tissue. While in the case of primary sarcomas, follow-up treatment after sparing surgery often consists of irradiation of the operated area, when treating patients with for sarcoma occurring in a previously irradiated area, repeat radiotherapy of the of the same area is not recommended. The optimal type of treatment in such a case is mastectomy in this case.
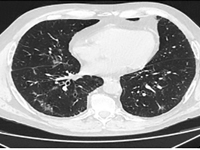
Infekcja SARS-CoV-2 u chorego na raka gruczołowego z mutacją w genie EGFR leczonego erlotynibem – opis przypadku
SARS-CoV-2 infection in a patient with adenocarcinoma with a mutation in the EGFR gene treated with erlotinib - a case report
Internal MedicineLung cancer accounts for the largest number of cancer deaths worldwide [1]. Despite advances in treatment, incidence and mortality rates continue to rise. A 2018 GLOBOCAN analysis reported 2.09 million new cases of lung cancer and 1.76 million deaths from lung cancer worldwide [2]. There are two main histological types: small cell lung cancer (DRP) and non-small cell lung cancer (NDRP). NDRP accounts for about 85% of all lung cancer cases. It includes various subtypes such as adenocarcinoma, squamous cell carcinoma and large cell carcinoma. The most common subtype is adenocarcinoma accounting for 45% of NDRP cases. The most important risk factor for developing lung cancer is smoking, especially among the male population. The use of filtered cigarettes, which reduce the amount of tar entering the lungs, correlates with an increase in the incidence of lung adenocarcinoma, which is associated with stronger inhalation of carcinogens into the fine airways. Other compounds that may have an effect on cancer development are asbestos, radon, nickel, cadmium, chromium, silica and arsenic. The development of molecular studies at the beginning of the 20th century made it possible to identify the genetic basis of the disease by demonstrating the presence of mutations or rearrangements of TP53, MYC, BCL2 genes in small cell carcinoma and EGFR, KRAS, MET, BRAF, NTRK, ROS1, ALK, RET, PIK3CA genes in non-small cell carcinoma [3]. The percentage of non-squamous NDRP patients with mutations in the gene for the epidermal growth factor receptor (EGFR) is 10-15 (in Caucasian patients) to more than 40% (in Asian patients) [4]. A deletion in exon 19 and a substitution at codon 858 (L858R) in exon 21 account for 80-90% of mutations within the tyrosine kinase coding domain of the EGFR gene [4]. Lung cancer manifests as cough, hemoptysis, chest pain, shortness of breath and/or hoarseness. In the case of adenocarcinoma, brain metastases manifesting as headache, vomiting, visual field disturbances, seizures or neurological deficits are common. After appropriate laboratory and imaging tests and histopathological evaluation, it is possible to assess the histological type and stage of the cancer. Depending on the patient's general condition, tumor stage and concomitant diseases, different treatment methods are used. For low-grade cancer (stages I, II and IIIA), surgery is used, often in combination with chemotherapy and radiation therapy. For stage IIIB patients, the therapy of choice is chemoradiotherapy, and if chemoradiotherapy is not available, the treatment is the same as for patients with generalized NDRP. Therapy for patients with distant metastases (stage IV) is aimed at reducing the discomfort and symptoms of progressive disease and prolonging life. For this purpose, chemotherapy, immunotherapy or molecularly targeted therapy are used [5]. Molecularly targeted therapy for lung cancer with EGFR gene mutations is made possible by the use of tyrosine kinase inhibitors (IKTs). IKTs inhibit intracellular phosphorylation of EGFR which leads to the arrest of cell differentiation, proliferation and angiogenesis. EGFR IKTs are divided into three generations. Erlotinib and gefitinib are the first-generation reversible IKTs. They are effective in the presence of the most common mutations in exon 19 and 21. Second-generation irreversible IKTs, which include afatinib and dacomitinib, show a broader spectrum of action. They block the transmission of signals formed by ErbB1 (EGFR), ErbB2 (HER2), ErbB3 and ErbB4 receptors, and can be effective in the presence of rare mutations in exons 18, 19, 20 and 21. It is possible to acquire resistance to first- and second-generation IKTs. Ozymertinib, an irreversible third-generation IKT, by acting on cells with the T790M mutation in exon 20 of the EGFR gene, overcomes resistance to treatment with older-generation EGFR IKTs, but can also be used in 1st-line treatment in NDRP patients regardless of the type of mutation in exons 18-21 of the EGFR gene [6]. The global COVID-19 pandemic poses a therapeutic challenge to healthcare, especially among oncology patients. A retrospective analysis from Wuhan showed that the risk of COVID-19 infection was 2.31 times higher among cancer patients than in healthy individuals. Smoking, age, male gender, cancer status, poor performance status (≥2 on the ECOG scale) and treatment with hydroxychloroquine with azithromycin were risk factors for increased 30-day mortality among COVID-19 patients [7]. Hospital visits during the pandemic and the use of immunosuppressive medications are major contributors to COVID-19 infection in lung cancer patients [8]. A study conducted in China, showed that NDRP patients over 60 years of age are particularly vulnerable to COVID-19 infection and a more severe course of the disease. Many respiratory symptoms in COVID-19 i.e. shortness of breath, cough, fever overlap with those of lung cancer. This creates a difficulty in differential diagnosis between the two disease entities. The diagnosis of COVID-19 is usually made on the basis of clinical history and PCR test and/or antigen test in a sample from nasopharyngeal secretions. Recognition of typical lesions seen on chest CT scan is also helpful. Multifocal opacities of the frosted-glass type with predilection for the lower lobes are present in 75% of patients [9]. A study conducted in New York among lung cancer patients with concurrent SARS-CoV2 infection showed the need for hospitalization in 62% of patients, 21% of whom required ICU hospitalization. Of the 102 patients participating in the study, 25% died. Survival was more dependent on the comorbidity of COPD (chronic obstructive pulmonary disease) and smoking than on tumor histology or PD-L1 (programmed death ligand 1) expression on tumor cells [10].

Przykład postępowania w przypadku guza II kości śródstopia pierwotnie podejrzewanego jako przerzut raka pęcherzykowatego tarczycy 40 i 20 lat po całkowitej tyroidektomii
Example of management of metatarsal bone II tumor originally suspected of having metastatic thyroid follicular cancer 40 and 20 years after total thyroidectomy
GynecologyKnown There are many causes causing discomfort and nodular lesions in the metatarsal area and forefoot. They include These include traumatic soft tissue injuries i bones (e.g., sole plate tears, toe arthritis, arthritis, fractures fatigue, Freiberg fracture), tendon diseases (e.g. tendinosis, tendon sheath inflammation, tendon rupture), non-cancerous soft tissue lesions (e.g., ganglion, bursitis bursitis, granuloma, Morton's neuroma), and, less commonly, tumors and their metastases to soft tissues and bone [1]. Focal bone lesions are often an incidental result of imaging. Alternatively, they may be the cause of pain, a palpable mass or a fracture pathological [2].Most often patients associate these symptoms with trauma. In fact, trauma only draws attention to the the affected area, but does not cause the formation of a tumor. [5] In all these cases, especially in the early stages, accurate diagnosis is crucial, to establish further differential diagnosis and treatment strategy, so when confronted with a focal bone lesion, it is necessary to follow a logical management algorithm. First, it should provide description of the lesion in correlation with the patient's age, location, type of bone, cortical involvement, periosteal reactions, the condition of the adjacent soft tissue. W this for this purpose, it is necessary to x-ray of the involved area in two projections with adjacent joints. A deeper diagnosis is achieved by CT examination, assessing the advancement of the bone lesions and MRI, infiltrating adjacent soft tissues . If imaging studies show more advanced disease, an important diagnostic element is to obtain material for pathomorphology, taken during open biopsy or oligobiopsy, and establish the histological diagnosis [11]. W case of confirmation of a neoplastic process, it is always necessary to perform a examination X-RAY/CT chest, ultrasound/ CT of the abdomen, or even PET to exclude metastases [5]. The second step of the implemented algorithm dictates that treatment should be planned based on the answers to the following questions: - Is the lesion likely to be a normal variant, That is, "leave me alone, don't touch me," a lesion of a benign type, requiring no further imaging or supplies, but only observation? [3] - Does the lesion have features suggestive of an aggressive nature, and then whether further imaging is necessary, which technique best to use, whether a biopsy of the lesion is required and advanced treatment? [4]. Heterogeneity clinical picture of unidentified focal nodular lesions w metatarsal and forefoot, the variety of available methods of diagnosis do not make the task any easier, both at the stage of making the initial diagnosis, as well as during communication between members of the interdisciplinary team, which many times should deal with address treatment. The purpose of of this article is to present a similar situation using the case of a tumor of the distal epiphysis of the second metatarsal bone as an example, suspected of late, distant metastasis of thyroid cancer, never not confirmed in further studies, and suggestions for management diagnostic and therapeutic management. Cancer Follicular The thyroid gland (FTC - Follicular Thyroid Carcinoma) accounts for 10-20% of of all cancers of the thyroid gland. It is the second most common encountered thyroid cancer [6], and metastasis to the metatarsal bones and fingers are extremely rare.

Radykalna radioterapia konformalna w leczeniu nawracającej, pozasutkowej postaci choroby Pageta - opis przypadku.
Radical conformal radiotherapy in treatment of recurrent, extramammary Paget disease - case report.
Internal MedicineDisease Paget's disease is a rare neoplastic process originating in the glands of the apocrine and eccrine glands of the skin [1]. A distinction is made between the mammary Paget disease (MPD) form and the extramammary Paget disease (EMPD), accounting for 90% and 10% of all cases, respectively Paget disease [2]. The incidence of EMPD in the European population is estimated to be is estimated at 0.7 per 100,000 people/year [3]. EMPD is more often diagnosed in women, particularly Caucasian, between the ages of 50 and 80. [4], in whom it mostly localizes on the vulva and perineum and in the perianal area, while in men on the penis and scrotal sac [5,6]. The symptoms of the disease are uncharacteristic, which in most cases makes it difficult to make a correct diagnosis and thus prolongs the time to start treatment. Only histopathologic examination of the excised lesion allows a correct diagnosis and an assessment of the degree of invasiveness of the process [6]. The primary method of treatment remains radical surgery [7]. Due to the high recurrence rate [4,8], some patients require follow-up treatment [6]. In cases ineligible for surgery, local or systemic chemotherapy or radiation therapy is used [9,10].Given the very rare occurrence of the disease, the lack of established treatment regimens, observed failures and subsequent attempts at surgical intervention, the case presented here is an example of the possibility of treating EMPD with ionizing radiation.